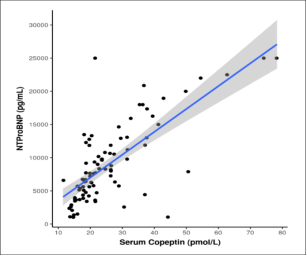
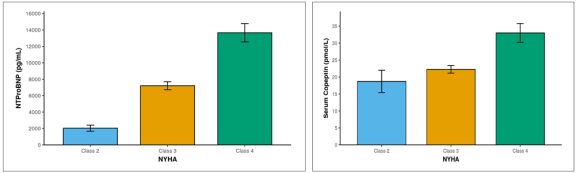
Introduction: Heart Failure is a leading cause of morbidity and mortality worldwide. It is associated with upregulation and dysfunction of the renin-angiotensin aldosterone system, the sympathetic nervous system and the vasopressin system. In heart failure, the levels of vasopressin are elevated and out of sync with the osmotic status. Arginine Vasopressin has a half-life of only 20 minutes and is bound to circulating platelets. Hence, it is not useful as a biomarker. Copeptin, a by-product of vasopressin metabolism has been used as a surrogate marker for Arginine Vasopressin in clinical practice. Thus, our study aims to find the use of copeptin in studying heart failure and its use in predicting severity. We also sought to correlate copeptin with NTproBNP the standard biomarker used in heart failure. Methods: Our study was a single-centre cross-sectional observational study involving 90 admitted heart failure patients over 18 months. NYHA Class was used to assess the severity of heart failure. Copeptin levels were measured using Human Copeptin ELISA Kit. Results: In these patients, elevated levels of copeptin and NTproBNP were found. In patients with higher NYHA Class, a greater rise in serum copeptin and NTproBNP levels was noted. Moreover, a strong positive correlation between NTproBNP and copeptin (rho = 0.7) was found in our study. Conclusion: Our study puts forward copeptin as a simple additional cost-effective biomarker for predicting the severity of heart failure.
| Published in | American Journal of Laboratory Medicine (Volume 9, Issue 4) |
| DOI | 10.11648/j.ajlm.20240904.12 |
| Page(s) | 45-49 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Heart Failure, Copeptin, NTproBNP, Severity, Arginine Vasopressin
Parameters | NYHA | p value | ||
|---|---|---|---|---|
Class 2 (n = 9) | Class 3 (n = 49) | Class 4 (n = 32) | ||
Age (years) | 56.67 ± 18.75 | 56.33 ± 12.15 | 61.56 ± 11.66 | 0.1221 |
Age | 0.1632 | |||
21-30 Years | 1 (11.1%) | 2 (4.1%) | 1 (3.1%) | |
31-40 Years | 1 (11.1%) | 3 (6.1%) | 1 (3.1%) | |
41-50 Years | 0 (0.0%) | 9 (18.4%) | 2 (6.2%) | |
51-60 Years | 3 (33.3%) | 17 (34.7%) | 7 (21.9%) | |
61-70 Years | 2 (22.2%) | 12 (24.5%) | 14 (43.8%) | |
71-80 Years | 1 (11.1%) | 6 (12.2%) | 7 (21.9%) | |
81-90 Years | 1 (11.1%) | 0 (0.0%) | 0 (0.0%) | |
Gender*** | 0.0433 | |||
Male | 3 (33.3%) | 37 (75.5%) | 21 (65.6%) | |
Female | 6 (66.7%) | 12 (24.5%) | 11 (34.4%) | |
NYHA Weighted Score*** | 2.00 ± 0.00 | 3.00 ± 0.00 | 4.00 ± 0.00 | <0.0011 |
NTProBNP (pg/mL)*** | 2039.89 ± 1112.20 | 7211.98 ± 3424.70 | 13662.00 ± 6329.43 | <0.0011 |
Serum Copeptin (pmol/L)*** | 18.72 ± 9.88 | 22.28 ± 7.93 | 33.01 ± 15.61 | <0.0011 |
Hemoglobin (mg/dL) | 10.73 ± 2.70 | 10.97 ± 1.87 | 10.61 ± 2.00 | 0.6771 |
Platelet Count (x10³/mm³) | 153.22 ± 73.83 | 205.23 ± 80.99 | 203.03 ± 85.74 | 0.1521 |
TLC (/mm³) | 6888.67 ± 1482.01 | 6913.45 ± 2321.54 | 6906.25 ± 2527.90 | 0.9751 |
S. Sodium (mEq/L) | 134.78 ± 5.56 | 136.51 ± 4.45 | 138.34 ± 5.35 | 0.1811 |
S. Potassium (mEq/L) | 4.06 ± 0.61 | 4.30 ± 0.51 | 4.47 ± 0.63 | 0.2281 |
S. Urea (mg/dL)*** | 46.78 ± 20.63 | 51.65 ± 23.50 | 75.91 ± 47.63 | 0.0181 |
S. Creatinine (mg/dL) | 0.77 ± 0.44 | 0.84 ± 0.65 | 1.35 ± 1.25 | 0.1381 |
S. Total Bilirubin (mg/dL)*** | 0.48 ± 0.19 | 0.71 ± 0.26 | 1.14 ± 0.85 | 0.0011 |
SGOT (U/L) | 56.11 ± 34.40 | 67.80 ± 63.75 | 316.62 ± 751.76 | 0.2671 |
SGPT (U/L) | 118.78 ± 223.07 | 65.24 ± 104.98 | 209.91 ± 457.50 | 0.7181 |
ALP (U/L) | 141.00 ± 85.81 | 110.37 ± 38.19 | 115.16 ± 47.88 | 0.8331 |
Ejection Fraction (%) | 36.50 ± 9.19 | 33.18 ± 10.06 | 25.38 ± 10.89 | 0.0691 |
Correlation | Spearman Correlation Coefficient | P Value |
|---|---|---|
Serum Copeptin (pmol/L) vs NTProBNP (pg/mL) | 0.7 | <0.001 |
RAAS | Renin Angiotensin Aldosterone System |
AVP | Arginine Vasopressin |
NTproBNP | N-terminal Pro-B type Natriuretic Peptide |
NYHA | New York Heart Association |
ELISA | Enzyme Linked Immunoassay |
| [1] | Savarese G, Lund LH, Division of Cardiology, Department of Medicine, Karolinska Insitutet, Stockholm, Sweden, Department of Cardiology, Karolinska University Hospital, Stockholm, Sweden, Global public health burden of heart failure. Card Fail Rev. 2017; 03(01): 7. |
| [2] | Huffman, Prabhakaran D. Heart failure: epidemiology and prevention in India. Natl Med J India. 2010; 23(5). |
| [3] | Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2022; 145(18). |
| [4] | Hartupee J, Mann DL. Neurohormonal activation in heart failure with reduced ejection fraction. Nat Rev Cardiol. 2017; 14(1): 30–8. |
| [5] | Singh RG. The physiology and emerging roles of antidiuretic hormone. Int J Clin Pract. 2002; 56(10). |
| [6] | Chatterjee K. Neurohormonal activation in congestive heart failure and the role of vasopressin. Am J Cardiol. 2005; 95(9): 8-13. |
| [7] | Schrier RW, Berl T, Anderson RJ. Osmotic and nonosmotic control of vasopressin release. Am J Physiol. 1979; 236(4): 321-32. |
| [8] | Robertson GL, Mahr EA, Athar S, Sinha T. Development and clinical application of a new method for the radioimmunoassay of arginine vasopressin in human plasma. J Clin Invest. 1973; 52(9): 2340–52. |
| [9] | Smyth DG, Massey DE. A new glycopeptide in pig, ox and sheep pituitary. Biochem Biophys Res Commun. 1979; 87(4): 1006–10. |
| [10] | Katan M, Müller B, Christ-Crain M. Copeptin: a new and promising diagnostic and prognostic marker. Crit Care. 2008; 12(2): 117 |
| [11] | Solà E, Kerbert AJC, Verspaget HW, Moreira R, Pose E, Ruiz P, et al. Plasma copeptin as biomarker of disease progression and prognosis in cirrhosis. J Hepatol. 2016; 65(5): 914–20 |
| [12] | Stoiser B, Mörtl D, Hülsmann M, Berger R, Struck J, Morgenthaler NG, et al. Copeptin, a fragment of the vasopressin precursor, as a novel predictor of outcome in heart failure. Eur J Clin Invest. 2006; 36(11): 771–8. |
| [13] | Gegenhuber A, Struck J, Dieplinger B, Poelz W, Pacher R, Morgenthaler NG, et al. Comparative evaluation of B-type natriuretic peptide, mid-regional pro-A-type natriuretic peptide, mid-regional pro-adrenomedullin, and copeptin to predict 1-year mortality in patients with acute destabilized heart failure. J Card Fail. 2007; 13(1): 42–9. |
| [14] | Tentzeris I, Jarai R, Farhan S, Perkmann T, Schwarz MA, Jakl G, et al. Complementary role of copeptin and high-sensitivity troponin in predicting outcome in patients with stable chronic heart failure. Eur J Heart Fail. 2011; 13(7): 726–33. |
| [15] | Neuhold S, Huelsmann M, Strunk G, Stoiser B, Struck J, Morgenthaler NG, et al. Comparison of copeptin, B-type natriuretic peptide, and amino-terminal pro-B-type natriuretic peptide in patients with chronic heart failure: prediction of death at different stages of the disease. J Am Coll Cardiol. 2008; 52(4): 266–72. |
| [16] | Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol. 2005; 95(8): 948–54. |
| [17] | Morgenthaler NG, Struck J, Alonso C, Bergmann A. Assay for the measurement of copeptin, a stable peptide derived from the precursor of vasopressin. Clin Chem. 2006; 52(1): 112–9. |
| [18] | Bhandari SS, Loke I, Davies JE, Squire IB, Struck J, Ng LL. Gender and renal function influence plasma levels of copeptin in healthy individuals. Clin Sci. 2009; 116(3): 257–63. |
| [19] | Masson S, Latini R, Carbonieri E, Moretti L, Rossi MG, Ciricugno S, et al. The predictive value of stable precursor fragments of vasoactive peptides in patients with chronic heart failure: data from the GISSI-heart failure (GISSI-HF) trial. Eur J Heart Fail. 2010; 12(4): 338–47. |
APA Style
Sen, R., Thakur, M. B., Rani, A. (2024). Correlation Between Serum Copeptin and NTproBNP Levels in Heart Failure. American Journal of Laboratory Medicine, 9(4), 45-49. https://doi.org/10.11648/j.ajlm.20240904.12
ACS Style
Sen, R.; Thakur, M. B.; Rani, A. Correlation Between Serum Copeptin and NTproBNP Levels in Heart Failure. Am. J. Lab. Med. 2024, 9(4), 45-49. doi: 10.11648/j.ajlm.20240904.12
@article{10.11648/j.ajlm.20240904.12,
author = {Rudra Sen and Manisha Bais Thakur and Anita Rani},
title = {Correlation Between Serum Copeptin and NTproBNP Levels in Heart Failure
},
journal = {American Journal of Laboratory Medicine},
volume = {9},
number = {4},
pages = {45-49},
doi = {10.11648/j.ajlm.20240904.12},
url = {https://doi.org/10.11648/j.ajlm.20240904.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20240904.12},
abstract = {Introduction: Heart Failure is a leading cause of morbidity and mortality worldwide. It is associated with upregulation and dysfunction of the renin-angiotensin aldosterone system, the sympathetic nervous system and the vasopressin system. In heart failure, the levels of vasopressin are elevated and out of sync with the osmotic status. Arginine Vasopressin has a half-life of only 20 minutes and is bound to circulating platelets. Hence, it is not useful as a biomarker. Copeptin, a by-product of vasopressin metabolism has been used as a surrogate marker for Arginine Vasopressin in clinical practice. Thus, our study aims to find the use of copeptin in studying heart failure and its use in predicting severity. We also sought to correlate copeptin with NTproBNP the standard biomarker used in heart failure. Methods: Our study was a single-centre cross-sectional observational study involving 90 admitted heart failure patients over 18 months. NYHA Class was used to assess the severity of heart failure. Copeptin levels were measured using Human Copeptin ELISA Kit. Results: In these patients, elevated levels of copeptin and NTproBNP were found. In patients with higher NYHA Class, a greater rise in serum copeptin and NTproBNP levels was noted. Moreover, a strong positive correlation between NTproBNP and copeptin (rho = 0.7) was found in our study. Conclusion: Our study puts forward copeptin as a simple additional cost-effective biomarker for predicting the severity of heart failure.
},
year = {2024}
}
TY - JOUR T1 - Correlation Between Serum Copeptin and NTproBNP Levels in Heart Failure AU - Rudra Sen AU - Manisha Bais Thakur AU - Anita Rani Y1 - 2024/11/11 PY - 2024 N1 - https://doi.org/10.11648/j.ajlm.20240904.12 DO - 10.11648/j.ajlm.20240904.12 T2 - American Journal of Laboratory Medicine JF - American Journal of Laboratory Medicine JO - American Journal of Laboratory Medicine SP - 45 EP - 49 PB - Science Publishing Group SN - 2575-386X UR - https://doi.org/10.11648/j.ajlm.20240904.12 AB - Introduction: Heart Failure is a leading cause of morbidity and mortality worldwide. It is associated with upregulation and dysfunction of the renin-angiotensin aldosterone system, the sympathetic nervous system and the vasopressin system. In heart failure, the levels of vasopressin are elevated and out of sync with the osmotic status. Arginine Vasopressin has a half-life of only 20 minutes and is bound to circulating platelets. Hence, it is not useful as a biomarker. Copeptin, a by-product of vasopressin metabolism has been used as a surrogate marker for Arginine Vasopressin in clinical practice. Thus, our study aims to find the use of copeptin in studying heart failure and its use in predicting severity. We also sought to correlate copeptin with NTproBNP the standard biomarker used in heart failure. Methods: Our study was a single-centre cross-sectional observational study involving 90 admitted heart failure patients over 18 months. NYHA Class was used to assess the severity of heart failure. Copeptin levels were measured using Human Copeptin ELISA Kit. Results: In these patients, elevated levels of copeptin and NTproBNP were found. In patients with higher NYHA Class, a greater rise in serum copeptin and NTproBNP levels was noted. Moreover, a strong positive correlation between NTproBNP and copeptin (rho = 0.7) was found in our study. Conclusion: Our study puts forward copeptin as a simple additional cost-effective biomarker for predicting the severity of heart failure. VL - 9 IS - 4 ER -
Department of Medicine, Vardhaman Mahavir Medical College and Safdarjung Hospital, New Delhi, India
Department of Medicine, Vardhaman Mahavir Medical College and Safdarjung Hospital, New Delhi, India
Department of Biochemistry, Vardhaman Mahavir Medical College and Safdarjung Hospital, New Delhi, India
Information