Gastrointestinal tuberculosis accounts for 1% to 3 % of all TB cases worldwide. Colonic tuberculosis is rare and can be mistaken for malignancy. It commonly presents as chronic abdominal pain along with night sweats, diarrhea, and fatigue and can resemble variety of other diseases making the diagnosis difficult. It presents with vague clinical and radiological picture making the diagnosis challenging for the clinicians. Its diagnosis is usually made by combining clinical features, radiological, tissue AFP staining and histopathologal examinations. The typical histopathologic findings include confluent large granulomas and langhans giant cells with caseating necrosis. Gastrointestinal tuberculosis responds well to standard antituberculous drugs and surgery is done for patients that have complications like strictures or obstruction which does not respond to medical therapy. This case illustrates a 40 year old man who presented with crampy lower abdominal pain and diagnosed as a colonic cancer both on imaging and clinically which later found to have colonic tuberculosis on a colectomy histopathologic sample. He was treated with anti-TB and respond well to his treatment. This case will give an insight for treating physicians to have a high index of suspicion for colonic TB in a patient who presented with lower abdominal pain and having colonic mass.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Chakinala RC, Khatri AM. Gastrointestinal Tuberculosis. Stat Pearls. Treasure Island (FL): StatPearls Publishing, 2021.
[1, 2]
. It can enter the GI tract through hematogenous route from active pulmonary TB, as a primary infection, through contiguous spread or through lymphatic channels and occur in any part of gastrointestinal tract with preference to the iliocaecal region
[3]
Uma Debi, Vasudevan Ravisankar, Kaushal Kishor Prasad, Saroj Kant Sinha, Arun Kumar Sharma World journal of gastroenterology, Abdominal tuberculosis of gastrointestinal tract: 2014, 14832-14839.
[3]
. It typically presents with vague clinical, radiological and histopathologic findings that resembles inflammatory bowel disease and malignancy thus making the diagnosis challenging
[4]
Alvares JF, Devarbhavi H, Makhija P, Rao S, Kottoor R: Clinical, colonoscopic, and histological profile of colonic tuberculosis in a tertiary hospital. Endoscopy; 2005; 37(4): 351–6.
[4]
. Gastrointestinal tuberculosis responds well to standard antituberculous drugs and surgery is done for patients that have complications like strictures or obstruction which does not respond to medical therapy
Elroy Patrick Weledji and Benjamin Thumamo Pokam, Abdominal tuberculosis: Is there a role for surgery? World journal of gastroenterology 2017; 174-181.
[6]
American Thoracic Society C, Infectious Diseases Society of America Treatment of tuberculosis. 2003; 52: 1–77.
[1, 5, 6].
2. Case Report
A 40 years old male presented with crampy lower abdominal pain of 3 years duration which is associated with intermittent watery diarrhea, loss of appetite and significant weight loss.
Physical exam
General appearance - he was emaciated with stable vital signs. There was conjuctival pallor and mild tenderness on the right lower quadrant of the abdomen.
Investigation
Complete blood count revealed mild anemia with Hemoglobin level of 10 g/dl.
Abdominal ultrasound showed intermediate segment ascending colon and hepatic flexure asymmetric circumferential nodular wall thickening with lost gut stratification with multiple paracholic and mesenteric enlarged lymph nodes and was highly suggestive of colonic cancer.
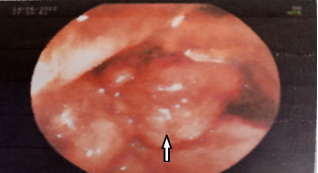
Colonoscopy revealed circumferential mass noted at 68 cm from anal verge the scope could not negotiate across the mass with the conclusion of ?Colonic cancer colonoscopic biopsy was done and showed chronic nonspecific inflammation with no features of malignancy, with differential diagnosis of Inflammatory bowel disease and Tuberculosis.
Figure 1. Constricting polypoid intraluminal mass (white arrow).
Despite negative colonoscopic biopsies, a provisional diagnosis of right colonic cancer was made and he was prepared for extended right hemicolectomy.
On laparotomy there was a long segment right colon mass extending from mid ascending colon up to hepatic flexure and multiple palpable mesenteric lymphnodes with minimal ascetic fluid. Hence, a right extended right hemicolectomy was performed with iliotransverse anastomosis and the specimen was sent for pathology for examination.
Histopathology evaluation
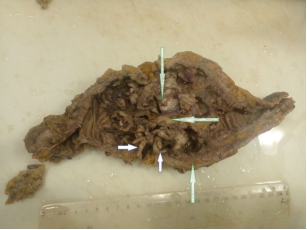
On gross examination there was a right hemicolectomy specimen measuring 28 cm long with numerous pedunculated polyps largest measuring 4 cm and constricting 3 x 1 cm mass on mid ascending colon with thickened bowel wall and 28 lymph nodes were identified (figure 2).
Figure 2. 28 cm long right hemicolectomy specimen with numerous pedunculated polyps (shorter arrow) and 3 x 1 cm constricting mass on mid ascending colon with thickened bowel wall (longer arrow).
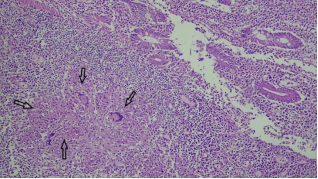
Figure 3. Granulomas and langhans giant cells (arrows), mononuclear inflammatory cells and ulcerated colonic mucosa.
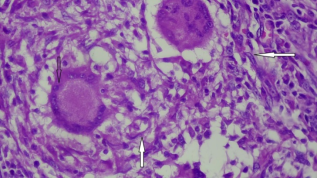
Microscopic evaluation of the thickened bowel wall and polyps showed polypoid colonic tissues containing glands lined by bland columnar epithelium with sub epithelial mononuclear inflammatory infiltrates including lymphocytes and plasma cells, numerous granulomas, langhans type giant cells and caseous necrosis (figures 3 and 4). Sections from the lymph nodes showed capsulated lymphoid tissue containing lymphoid follicles numerous granulomas, langhans type giant cells and caseous necrosis figure 5. There were no features of malignancy that were seen.
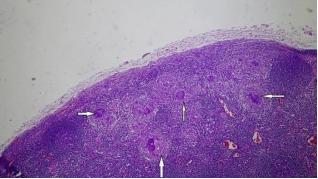
Figure 5. H&E -low power view of a Lymph node with multiple granulomas and giant cells (white arrow).
3. Treatment
With the diagnosis of Disseminated Tuberculosis to the colon and lymphnode he was started on Rifampicin (10 mg/kg/d), Isoniazid (5 mg/kg/d), Pyrazinamide (30 mg/kg/d) and Ethambutol (15 mg/kg/d) he is currently on follow-up and is responding to the anti TB treatment.
4. Discussion
Gastrointestinal tuberculosis is a relatively uncommon form of TB with isolated involvement of colon in 10.8% of cases
[7]
Lau CF, et al. A case of colonic tuberculosis mimicking Crohn's disease. Hong Kong Medical Journal 4(1998): 63-66.
[7]
. It is the major health problem in the developing countries with the rising numbers in immunocompromised patients and patients with HIV virus
[3]
Uma Debi, Vasudevan Ravisankar, Kaushal Kishor Prasad, Saroj Kant Sinha, Arun Kumar Sharma World journal of gastroenterology, Abdominal tuberculosis of gastrointestinal tract: 2014, 14832-14839.
[3]
. TB is also a concern in patients receiving biological agents for conditions like inflammatory bowel disease and rheumatoid arthritis. It commonly presents as chronic abdominal pain along with night sweats, diarrhea, and fatigue and can resemble variety of other diseases making the diagnosis difficult. Its diagnosis is usually made by combining clinical features, radiological, tissue AFP staining and histopathologal examinations
Uma Debi, Vasudevan Ravisankar, Kaushal Kishor Prasad, Saroj Kant Sinha, Arun Kumar Sharma World journal of gastroenterology, Abdominal tuberculosis of gastrointestinal tract: 2014, 14832-14839.
[1, 3]
.
Microbiological examination to diagnose intestinal tuberculosis includes AFB and culture
[8]
Yun Jung Lee, Suk-Kyun Yang, Seung Jae Myung, “The usefulness of colonoscopic biopsy in the diagnosis of intestinal tuberculosis and pattern of concomitant extra-intestinal tuberculosis” The Korean journal of gastroenterology, vol. 44, no. 3, pp. 153-159, 2004.
[9]
Lowbridge, C., Fadhil, S. A. M., Krishnan, G. D. et al. How can gastro-intestinal tuberculosis diagnosis be improved? A prospective cohort study. BMC Infect Dis 20, 255(2020).
[8, 9]
. When they are done on stool or sputum they yield positive results in approximately 50 % of the time, and in intestinal TB biopsies AFB and MTB culture positivity are only found on 17% and 29% of the cases respectively in one large study
[8]
Yun Jung Lee, Suk-Kyun Yang, Seung Jae Myung, “The usefulness of colonoscopic biopsy in the diagnosis of intestinal tuberculosis and pattern of concomitant extra-intestinal tuberculosis” The Korean journal of gastroenterology, vol. 44, no. 3, pp. 153-159, 2004.
[8]
PCR for M. tuberculosis from biopsies also provides rapid diagnosis of TB and positive predictive values up to 100% have been reported
[10]
R. S. Wiener, P. Della-Latta, and N. W. Schluger, “Effect of nucleic acid amplification for Mycobacterium tuberculosis on clinical decision making in suspected extrapulmonary tuberculosis,” Chest, vol. 128, no. 1, pp. 102–107, 2005.
[10]
.
Radiologic imaging plays an important part in diagnosis with most common feature being mural thickening in 93 % of the cases. Other features include mesenteric adenopathy, inflammatory pseudopolyps, deformity of Ileocecal Valve and Stenosis
[3]
Uma Debi, Vasudevan Ravisankar, Kaushal Kishor Prasad, Saroj Kant Sinha, Arun Kumar Sharma World journal of gastroenterology, Abdominal tuberculosis of gastrointestinal tract: 2014, 14832-14839.
[11]
Dong Ho Lee, MD, Young Tae Ko, MD, Yup Yoon, MD, Jae Hoon Lim, MD: Sonographic Findings of Intestinal Tuberculosis: 537-540.
[3, 11]
. Circumferential ulcers surrounded by inflamed mucosa are common colonoscopic features
[11]
Dong Ho Lee, MD, Young Tae Ko, MD, Yup Yoon, MD, Jae Hoon Lim, MD: Sonographic Findings of Intestinal Tuberculosis: 537-540.
[12]
S. Mukewar, R. Ravi, and A. Prasad, “Colon tuberculosis: endoscopic features and prospective endoscopic follow-up after anti-tuberculosis treatment,” Clinical and Translational Gastroenterology, vol. 3, 24 pages, 2012.
[11, 12]
.
The typical histopathologic findings include confluent large granulomas and langhans giant cells with caseating necrosis. In 55.5% Epithelioid cell granulomas were seen in the mucosal layer of the bowel wall and in 44.5% cases, the granulomas were present deep to the mucosa with lymphoplasmocytic inflammation. Caseation may only be seen in lymph nodes or it may be totally absent in patients who have received anti tuberculosis in the past
P. B. Tripathi and A. D. Amarapurkar, “Morphological spectrum of gastrointestinal tuberculosis, Trop Gastroenterology”, Vol, 30, no. 1, pp. 35-39, 2009.
[1, 13]
.
The main stay of treatment of gastrointestinal tuberculosis is anti-microbial therapy (Rifampicin, Isoniazide, pyrazinamide and ethambutol for 2 months and Rifampicin and isoniazide for 4 months)
American Thoracic Society C, Infectious Diseases Society of America Treatment of tuberculosis. 2003; 52: 1–77.
[1, 6]
Surgery is essentially reserved for those with acute surgical complications including perforation, massive bleeding, complete obstruction, or obstruction not responding to medical management
[5]
Elroy Patrick Weledji and Benjamin Thumamo Pokam, Abdominal tuberculosis: Is there a role for surgery? World journal of gastroenterology 2017; 174-181.
[5]
.
This case illustrates not only a case of colonic tuberculosis but also a case mimicking a colonic cancer. It is essential to entertain a broad differential diagnosis when evaluating a patient with a colonic mass by paying a close attention to patient demographics and risk factors. Differentiating between tuberculosis and malignancy can be difficult talking into account that both entities may present themselves as a circumferential nodular wall thickening and multiple lymphadenopathies on imaging. Although in our case colonoscopic appearance was suggestive of a carcinoma, histology showed chronic inflammatory changes on colonoscopy biopsy’s and caseating epithelioid granulomas on colectomy sample, a pattern consistent with colonic Tuberculosis. It is important to maintain high index of clinical suspicion for Gastrointestinal Tuberculosis in developing countries and do biopsies to reach to early diagnosis and prevent unnecessary surgical intervention thus making the diagnosis multidisciplinary.
Abbreviations
TB
Tuberculosis
AFB
Acid Fast Bacillus
MTB
Mycobacterium Tuberculosis
GI
Gastro-Intestine
PCR
Polymerase Chain Reaction
Acknowledgments
The authors would like to acknowledge all the managing teams who participated in the betterment of this client and the accomplishment of this case report.
Funding
This is a hospital-based case report, with no funds or associated grants.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Chakinala RC, Khatri AM. Gastrointestinal Tuberculosis. Stat Pearls. Treasure Island (FL): StatPearls Publishing, 2021.
[3]
Uma Debi, Vasudevan Ravisankar, Kaushal Kishor Prasad, Saroj Kant Sinha, Arun Kumar Sharma World journal of gastroenterology, Abdominal tuberculosis of gastrointestinal tract: 2014, 14832-14839.
[4]
Alvares JF, Devarbhavi H, Makhija P, Rao S, Kottoor R: Clinical, colonoscopic, and histological profile of colonic tuberculosis in a tertiary hospital. Endoscopy; 2005; 37(4): 351–6.
[5]
Elroy Patrick Weledji and Benjamin Thumamo Pokam, Abdominal tuberculosis: Is there a role for surgery? World journal of gastroenterology 2017; 174-181.
[6]
American Thoracic Society C, Infectious Diseases Society of America Treatment of tuberculosis. 2003; 52: 1–77.
[7]
Lau CF, et al. A case of colonic tuberculosis mimicking Crohn's disease. Hong Kong Medical Journal 4(1998): 63-66.
[8]
Yun Jung Lee, Suk-Kyun Yang, Seung Jae Myung, “The usefulness of colonoscopic biopsy in the diagnosis of intestinal tuberculosis and pattern of concomitant extra-intestinal tuberculosis” The Korean journal of gastroenterology, vol. 44, no. 3, pp. 153-159, 2004.
[9]
Lowbridge, C., Fadhil, S. A. M., Krishnan, G. D. et al. How can gastro-intestinal tuberculosis diagnosis be improved? A prospective cohort study. BMC Infect Dis 20, 255(2020).
[10]
R. S. Wiener, P. Della-Latta, and N. W. Schluger, “Effect of nucleic acid amplification for Mycobacterium tuberculosis on clinical decision making in suspected extrapulmonary tuberculosis,” Chest, vol. 128, no. 1, pp. 102–107, 2005.
[11]
Dong Ho Lee, MD, Young Tae Ko, MD, Yup Yoon, MD, Jae Hoon Lim, MD: Sonographic Findings of Intestinal Tuberculosis: 537-540.
[12]
S. Mukewar, R. Ravi, and A. Prasad, “Colon tuberculosis: endoscopic features and prospective endoscopic follow-up after anti-tuberculosis treatment,” Clinical and Translational Gastroenterology, vol. 3, 24 pages, 2012.
[13]
P. B. Tripathi and A. D. Amarapurkar, “Morphological spectrum of gastrointestinal tuberculosis, Trop Gastroenterology”, Vol, 30, no. 1, pp. 35-39, 2009.
Lucas, F. Y., Tadele, A. K., Engida, G. G., Geremew, T. T., Wodajo, A. A., et al. (2024). Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report. American Journal of Laboratory Medicine, 9(4), 41-44. https://doi.org/10.11648/j.ajlm.20240904.11
Lucas, F. Y.; Tadele, A. K.; Engida, G. G.; Geremew, T. T.; Wodajo, A. A., et al. Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report. Am. J. Lab. Med.2024, 9(4), 41-44. doi: 10.11648/j.ajlm.20240904.11
Lucas FY, Tadele AK, Engida GG, Geremew TT, Wodajo AA, et al. Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report. Am J Lab Med. 2024;9(4):41-44. doi: 10.11648/j.ajlm.20240904.11
@article{10.11648/j.ajlm.20240904.11,
author = {Fekade Yerakley Lucas and Abraham Kassahun Tadele and Ghion Getnet Engida and Teketel Tadesse Geremew and Abebaw Amare Wodajo and Melaku Teshale Gemechu and Menberu Moges Ayele and Kalkidan Molla Tegengne and Akmel Umer Ebrahim and Tigist Gutema Tesgera},
title = {Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report
},
journal = {American Journal of Laboratory Medicine},
volume = {9},
number = {4},
pages = {41-44},
doi = {10.11648/j.ajlm.20240904.11},
url = {https://doi.org/10.11648/j.ajlm.20240904.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20240904.11},
abstract = {Gastrointestinal tuberculosis accounts for 1% to 3 % of all TB cases worldwide. Colonic tuberculosis is rare and can be mistaken for malignancy. It commonly presents as chronic abdominal pain along with night sweats, diarrhea, and fatigue and can resemble variety of other diseases making the diagnosis difficult. It presents with vague clinical and radiological picture making the diagnosis challenging for the clinicians. Its diagnosis is usually made by combining clinical features, radiological, tissue AFP staining and histopathologal examinations. The typical histopathologic findings include confluent large granulomas and langhans giant cells with caseating necrosis. Gastrointestinal tuberculosis responds well to standard antituberculous drugs and surgery is done for patients that have complications like strictures or obstruction which does not respond to medical therapy. This case illustrates a 40 year old man who presented with crampy lower abdominal pain and diagnosed as a colonic cancer both on imaging and clinically which later found to have colonic tuberculosis on a colectomy histopathologic sample. He was treated with anti-TB and respond well to his treatment. This case will give an insight for treating physicians to have a high index of suspicion for colonic TB in a patient who presented with lower abdominal pain and having colonic mass.
},
year = {2024}
}
TY - JOUR
T1 - Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report
AU - Fekade Yerakley Lucas
AU - Abraham Kassahun Tadele
AU - Ghion Getnet Engida
AU - Teketel Tadesse Geremew
AU - Abebaw Amare Wodajo
AU - Melaku Teshale Gemechu
AU - Menberu Moges Ayele
AU - Kalkidan Molla Tegengne
AU - Akmel Umer Ebrahim
AU - Tigist Gutema Tesgera
Y1 - 2024/09/29
PY - 2024
N1 - https://doi.org/10.11648/j.ajlm.20240904.11
DO - 10.11648/j.ajlm.20240904.11
T2 - American Journal of Laboratory Medicine
JF - American Journal of Laboratory Medicine
JO - American Journal of Laboratory Medicine
SP - 41
EP - 44
PB - Science Publishing Group
SN - 2575-386X
UR - https://doi.org/10.11648/j.ajlm.20240904.11
AB - Gastrointestinal tuberculosis accounts for 1% to 3 % of all TB cases worldwide. Colonic tuberculosis is rare and can be mistaken for malignancy. It commonly presents as chronic abdominal pain along with night sweats, diarrhea, and fatigue and can resemble variety of other diseases making the diagnosis difficult. It presents with vague clinical and radiological picture making the diagnosis challenging for the clinicians. Its diagnosis is usually made by combining clinical features, radiological, tissue AFP staining and histopathologal examinations. The typical histopathologic findings include confluent large granulomas and langhans giant cells with caseating necrosis. Gastrointestinal tuberculosis responds well to standard antituberculous drugs and surgery is done for patients that have complications like strictures or obstruction which does not respond to medical therapy. This case illustrates a 40 year old man who presented with crampy lower abdominal pain and diagnosed as a colonic cancer both on imaging and clinically which later found to have colonic tuberculosis on a colectomy histopathologic sample. He was treated with anti-TB and respond well to his treatment. This case will give an insight for treating physicians to have a high index of suspicion for colonic TB in a patient who presented with lower abdominal pain and having colonic mass.
VL - 9
IS - 4
ER -
Lucas, F. Y., Tadele, A. K., Engida, G. G., Geremew, T. T., Wodajo, A. A., et al. (2024). Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report. American Journal of Laboratory Medicine, 9(4), 41-44. https://doi.org/10.11648/j.ajlm.20240904.11
Lucas, F. Y.; Tadele, A. K.; Engida, G. G.; Geremew, T. T.; Wodajo, A. A., et al. Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report. Am. J. Lab. Med.2024, 9(4), 41-44. doi: 10.11648/j.ajlm.20240904.11
Lucas FY, Tadele AK, Engida GG, Geremew TT, Wodajo AA, et al. Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report. Am J Lab Med. 2024;9(4):41-44. doi: 10.11648/j.ajlm.20240904.11
@article{10.11648/j.ajlm.20240904.11,
author = {Fekade Yerakley Lucas and Abraham Kassahun Tadele and Ghion Getnet Engida and Teketel Tadesse Geremew and Abebaw Amare Wodajo and Melaku Teshale Gemechu and Menberu Moges Ayele and Kalkidan Molla Tegengne and Akmel Umer Ebrahim and Tigist Gutema Tesgera},
title = {Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report
},
journal = {American Journal of Laboratory Medicine},
volume = {9},
number = {4},
pages = {41-44},
doi = {10.11648/j.ajlm.20240904.11},
url = {https://doi.org/10.11648/j.ajlm.20240904.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20240904.11},
abstract = {Gastrointestinal tuberculosis accounts for 1% to 3 % of all TB cases worldwide. Colonic tuberculosis is rare and can be mistaken for malignancy. It commonly presents as chronic abdominal pain along with night sweats, diarrhea, and fatigue and can resemble variety of other diseases making the diagnosis difficult. It presents with vague clinical and radiological picture making the diagnosis challenging for the clinicians. Its diagnosis is usually made by combining clinical features, radiological, tissue AFP staining and histopathologal examinations. The typical histopathologic findings include confluent large granulomas and langhans giant cells with caseating necrosis. Gastrointestinal tuberculosis responds well to standard antituberculous drugs and surgery is done for patients that have complications like strictures or obstruction which does not respond to medical therapy. This case illustrates a 40 year old man who presented with crampy lower abdominal pain and diagnosed as a colonic cancer both on imaging and clinically which later found to have colonic tuberculosis on a colectomy histopathologic sample. He was treated with anti-TB and respond well to his treatment. This case will give an insight for treating physicians to have a high index of suspicion for colonic TB in a patient who presented with lower abdominal pain and having colonic mass.
},
year = {2024}
}
TY - JOUR
T1 - Colonic Tuberculosis Mimicking Colonic Cancer: A Multidisciplinary Diagnosis and Case Report
AU - Fekade Yerakley Lucas
AU - Abraham Kassahun Tadele
AU - Ghion Getnet Engida
AU - Teketel Tadesse Geremew
AU - Abebaw Amare Wodajo
AU - Melaku Teshale Gemechu
AU - Menberu Moges Ayele
AU - Kalkidan Molla Tegengne
AU - Akmel Umer Ebrahim
AU - Tigist Gutema Tesgera
Y1 - 2024/09/29
PY - 2024
N1 - https://doi.org/10.11648/j.ajlm.20240904.11
DO - 10.11648/j.ajlm.20240904.11
T2 - American Journal of Laboratory Medicine
JF - American Journal of Laboratory Medicine
JO - American Journal of Laboratory Medicine
SP - 41
EP - 44
PB - Science Publishing Group
SN - 2575-386X
UR - https://doi.org/10.11648/j.ajlm.20240904.11
AB - Gastrointestinal tuberculosis accounts for 1% to 3 % of all TB cases worldwide. Colonic tuberculosis is rare and can be mistaken for malignancy. It commonly presents as chronic abdominal pain along with night sweats, diarrhea, and fatigue and can resemble variety of other diseases making the diagnosis difficult. It presents with vague clinical and radiological picture making the diagnosis challenging for the clinicians. Its diagnosis is usually made by combining clinical features, radiological, tissue AFP staining and histopathologal examinations. The typical histopathologic findings include confluent large granulomas and langhans giant cells with caseating necrosis. Gastrointestinal tuberculosis responds well to standard antituberculous drugs and surgery is done for patients that have complications like strictures or obstruction which does not respond to medical therapy. This case illustrates a 40 year old man who presented with crampy lower abdominal pain and diagnosed as a colonic cancer both on imaging and clinically which later found to have colonic tuberculosis on a colectomy histopathologic sample. He was treated with anti-TB and respond well to his treatment. This case will give an insight for treating physicians to have a high index of suspicion for colonic TB in a patient who presented with lower abdominal pain and having colonic mass.
VL - 9
IS - 4
ER -