Abstract
Laboratory investigations are an integral part of patient management. The number and frequency of investigations are directly related to the clinical seriousness of a patient. Hence acute care setups observe a high volume as well as frequency of sampling for laboratory analyses. Many management plans are dependent on the results of these investigations. So, there is also pressure on the pathology laboratory to provide the results as early as possible. The whole process of lab investigation requires ordering an investigation, sending the requisition/system indenture, sampling, transporting sample to the lab, analysing, result approval and sending/uploading the report. Well-planned, tried, and tested standards/ protocols must be in place in order to eliminate the probability of errors in investigation reports. Laboratories must work according to some set specifications in order to process the samples in an error free manner. This paper will analyse the procedural steps, scope of errors and steps to identify, report as well as rectify the errors in the pre-analytical phase of laboratory investigations in a highly demanding and accident-prone acute care setup. The aim of this exercise is to improve the quality of lab reporting process with an objective to eliminate pre analytic laboratory errors.
Keywords
Laboratory Investigations, Patient Management, Sampling, Pre-Analytical Phase
1. Introduction
1.1. Background of the Study
In acute care facilities, accurate and timely laboratory testing is critical for effective patient care. However, the reliability of laboratory results hinges on the integrity of the pre-analytic phase, which includes sample collection, handling, transportation, and processing.
Pre-analytic errors, ranging from mislabelled specimens to delays in processing, are prevalent in clinical laboratories and can lead to misdiagnosis and suboptimal patient outcomes. Acute care settings exacerbate these errors due to time constraints, high patient volumes, and emergent situations, which pressure laboratory staff and leave little room for error correction.
While strategies such as standard operating procedures and staff training aim to mitigate pre-analytic errors, their effectiveness in acute care setups is uncertain. Thus, there's a need for tailored approaches to address the unique challenges of these environments.
A case study offers a valuable opportunity to explore pre-analytic error management in acute care settings. By analyzing real-world scenarios, researchers can identify specific challenges, root causes, and opportunities for improvement. Implementing targeted interventions and evaluating their impact can provide actionable insights to enhance patient safety and laboratory efficiency.
The present study aims to conduct a comprehensive analysis of pre-analytic error occurrences, underlying factors, and interventions in an acute care setup. Through evidence-based recommendations, it seeks to contribute to efforts to improve the quality and reliability of laboratory testing in acute care settings.
1.2. Defining Lab Error – Common Versus Special Cause Variation
The first question arises is an objective criterion for defining an error. Any value of pathology lab report which is different from the actual value is considered as an error. But the biggest challenge is to know the actual value. It is almost impossible to know the actual value without relying on the lab analysis technology. And regular standardization of lab technology with controls is an important routine activity of NABL accredited labs. The laboratory analyses the concentration of blood components in a given case study.
Even the machines using the most advanced technology have some margin of error, which is documented in the product manual. Besides machines inherent margin of error, various other factors in pre-analytical and post analytical phase can lead to reports which might be significantly different from the actual value.
So, for all practical purposes, slight changes from the actual value can be considered as a common cause variation. Any significant discrepancy between either the two reports of same parameter or a report not correlating with the clinical condition of the patient leads to the special cause variation. This significant discrepancy, which is a special cause variation, needs further investigation for root cause analysis. So, lab errors are of two types:
1) Determinate or Systematic Error – Common Cause Variation
2) Indeterminate or Random Error – Special Cause Variation
Although no specific action is required for systematic errors, regular audit, maintenance, and standardization of method is important to keep the systematic errors in check. Our focus is to look for the incidence of random errors, which are mostly in pre-analytical phase of lab investigation process. These errors are caught based on suspicion.
2. Literature Review
In the dynamic landscape of healthcare delivery, acute care units in major Indian cities grapple with numerous challenges, hindering the delivery of high-quality care. From a pervasive lack of trust and escalating costs to overburdened staff and prolonged wait times, these issues underscore the urgent need for innovative solutions. This review explores the transformative potential of Lean culture, drawing insights from academic research, to address the complex challenges faced by acute care sections in these institutions.
Challenges in Acute Care Setup
The prevalence and types of pre-analytic errors, including mislabeled specimens, inadequate sample collection, and transportation mishaps, across various healthcare settings.
| [6] | Womack, J. P., Jones, D. T., & Roos, D. (1990). The Machine That Changed the World: The Story of Lean Production. Free Press. |
[6]
The heightened risk of pre-analytic errors in acute care environments due to time constraints and emergent situations.
| [7] | Shingo, S. (1986). Zero Quality Control: Source Inspection and the Poka-Yoke System. Productivity Press. |
[7]
The root causes and contributing factors associated with pre-analytic errors, including human factors (staff workload, fatigue), system-related issues (workflow inefficiencies, inadequate resources), and organizational factors (communication breakdowns, culture of blame).
| [8] | Radnor, Z., Holweg, M., & Waring, J. (2012). Lean in healthcare: The unfilled promise? Social Science & Medicine, 74(3), 364-371. |
[8]
Quality improvement initiatives play a vital role in addressing pre-analytic errors. These initiatives encompass a range of activities, including root cause analysis, performance monitoring, and implementation of corrective actions.
| [9] | Rother, M., & Shook, J. (1999). Learning to See: Value Stream Mapping to Add Value and Eliminate MUDA. The Lean Enterprise Institute. |
[9]
The significant impact of pre-analytic errors on patient care outcomes, such as misdiagnosis, inappropriate treatment, and compromised patient safety. Moreover, pre-analytic errors contribute to increased healthcare costs due to the need for repeated testing, unnecessary treatments, and potential litigation.
| [10] | Kenney, C., & Florida, R. (2004). Locating Global Advantage: Industry Dynamics in the International Economy. Stanford University Press. |
[10]
The strategies for detecting and preventing pre-analytic errors, including the implementation of standard operating procedures (SOPs), quality control measures, and staff training programs. The use of technology, such as barcode labelling systems and electronic medical record integration, has shown promise in reducing pre-analytic errors.
| [11] | Toussaint, J. S., & Berry, L. L. (2013). The Promise of Lean in Health Care. Mayo Clinic Proceedings, 88(1), 74-82. |
[11]
Automation and technology play a significant role in mitigating pre-analytic errors by standardizing processes and reducing manual interventions. Barcode systems for sample identification, automated specimen transport systems, and electronic ordering systems are examples of technological solutions that can improve the accuracy and efficiency of the pre-analytic phase.
| [12] | NHS Institute for Innovation and Improvement. (2007). The Lean Experience: A Story of Continuous Improvement. |
[12]
Case studies and real-world examples provide valuable insights into the practical challenges and interventions related to pre-analytic errors in acute care setups. These studies highlight the effectiveness of targeted interventions, such as process redesign, staff education, and technology implementation, in reducing pre-analytic errors and improving laboratory efficiency.
| [13] | Graban, M. (2012). Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement (2nd ed.). CRC Press. |
[13]
Education and training programs are essential for ensuring staff competency and adherence to standard procedures in the pre-analytic phase. Studies have shown that ongoing education and training initiatives can improve staff awareness of pre-analytic errors, leading to better error prevention and management practices.
| [14] | Womack, J. P., & Jones, D. T. (2003). Lean Thinking: Banish Waste and Create Wealth in Your Corporation. Free Press. |
[14]
Continuous monitoring and evaluation of pre-analytic processes are essential for identifying recurring errors and implementing targeted interventions. Regular audits, performance metrics, and feedback mechanisms enable laboratories to track error rates, assess the effectiveness of implemented measures, and drive ongoing improvements in quality and safety
| [15] | Radnor, Z. J., Holweg, M., & Waring, J. (2012). Lean in healthcare: The unfilled promise? Social Science & Medicine, 74(3), 364-371. |
[15]
.
3. Case Study
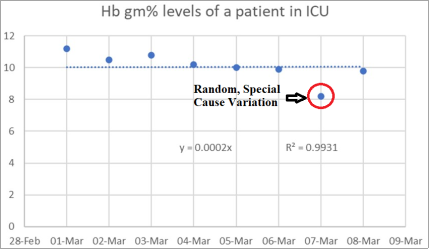
An elderly male was admitted with complaints of vomiting, diarrhoea, low blood pressure and kidney failure. He was managed in ICU, recovered completely, and discharged after 10 days of admission in the hospital. He showed very good response to management and his kidney failure reverted to normal by 6
th day of ICU management. However, his shifting out of ICU on 7
th day was put on hold due to an alarming haemoglobin report showing a fall of 2 gm%. (See
Figure 1).
Significant time, energy and money were spent on the patient to rule out any serious reason for this Hb fall. Lab error was suspected because on the next day, the report again shot back to normal, and patient was shifted out of ICU. Thus, a single lab error resulted in a lot of waste of time, energy, and resources to identify the reason of this “special cause variation”.
Figure 1. Chart showing the Hb levels of a patient admitted with complaints of vomiting, diarrhoea, low blood pressure and kidney failure. The trendline is showing a mean of 10 gm% with daily common variations. The last two readings of 7th and 8th March indicate significant variation, which does not correlate clinically.
4. Objective
The exercise is done with an aim to identify and eliminate pre-analytical lab errors falling in the category of special cause variation. The objectives are:
1) To identify the incidence rate of suspicious lab errors in an acute care setup (ICU & HDU)
2) Supervise the pre-analytical phase of lab investigation by Gemba walks and improve it by implementing the principles of lean.
3) Perform root cause analysis of the identified errors.
4) Standardize the pre-analytical phase.
5. Incidence
Four basic investigation parameters namely hemoglobin (Hb%), Creatinine (S.Cr), Sodium (S.Na) and Potassium (S.K) were selected to find the incidence of suspicious lab errors.
Table 1. Four Categories of Suspicious Lab Errors.
Normal values reported of an abnormal patient – e.g., Hb of 10 gm% reported of an anaemic patient. | Abnormal values reported of a normal patient – e.g., Hb of 8 gm% reported of a normal patient. |
More abnormal values reported of a less abnormal patient. – e.g., Hb of 6 gm% reported of a patient having Hb of 8 gm% | Less abnormal values are reported of a more abnormal patient – e.g., Hb of 8 gm% reported of a patient having Hb of 6 gm% |
The suspicious lab reports were reconfirmed with the pathology laboratory and resampling done after weighing the risks and benefits on case-to-case basis. All suspicious random variations were considered as lab errors if either or all the following Clinical Incongruency criteria were found:
1) Highly abnormal report in a clinically stable patient.
2) Normal report in a clinically sick and unstable patient.
3) Unjustified change from the prior report without any clinically evident reason.
After one week of data collection, it was found that the incidence of suspicious lab errors based on the above-mentioned criteria was 2.1%.
Observing the Process
Table 2.
Types and Rates of Error in the 3 Stages of the Laboratory Testing Process . Phase of Total Testing Process | Type of Error | Rates |
Pre-analytical | 1) Inappropriate test request 2) Order entry errors 3) Misidentification of patient 4) Container inappropriate 5) Sample collection and transport inadequate 6) Inadequate sample/anticoagulant volume ratio 7) Insufficient sample volume 8) Sorting and routing errors 9) Labelling errors | 46%-68.2% |
Analytical | 1) Equipment malfunction Sample mix-ups/interference 2) Undetected failure in quality control 3) Procedure not followed | 7%-13% |
Post-analytical | 1) Failure in reporting Erroneous validation of analytical data 2) Improper data entry | 18.5%-47% |
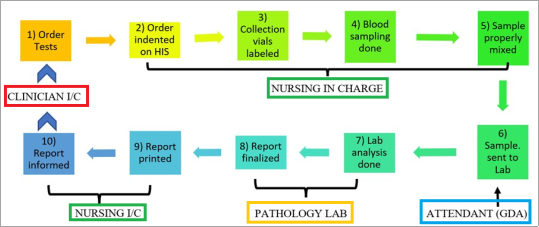
The whole pre-analytical process was observed to identify possible areas of errors. The process of laboratory investigation is classified broadly in three phases – pre-analytical, analytical, and post analytical. By scrutinizing the process of laboratory pathology, the errors can be classified as pre-analytic (46-68.2%), analytic (7%-13%) and post-analytic (18.5-45%)
| [2] | Halverson AL, Dintzis SM, Pavkovic S. 2016 Dec; "Surgical Specimen Management: A Descriptive Study of 648 Adverse Events and Near Misses." Arch Pathol Lab Med. 140(12): 1390-1396. |
[2]
.
Figure 2. Process chart of laboratory investigation and the delegated personnel.
6. The Standard Operating Procedure
The tests namely Hb, S.Na, S.K and S.Cr are part of the daily routine investigations of Complete Blood Count (CBC) and Kidney Function Tests (KFT) sent daily for the patient admitted in the ICU/ HDU.
STEP 1 - Test Order: The critical care consultant in the night duty cross checks whether any daily routine investigations (CBC, KFT) are to be withheld. The investigations to be sent on the day are finalized by 5 a.m.
STEP 2 – Test Indentation: The nursing staff confirms the ordered test with the nursing supervisor, who indents the test on Hospital Information System (HIS) software.
STEP 3 – Labelling of Collection Vials – The collection vials are labelled with the Name, Age, Gender, UHID No., IPD No., date, and time. The work is supervised by the nursing in-charge.
STEP 4 – Blood Sampling – 5 ml of blood is collected under strict aseptic precautions by the nursing staff and transferred in plain (red – 3 ml) and EDTA (purple – 2 ml) pre-labelled vacutainers. The EDTA vacutainers are rolled between the palms for 5-10 seconds.
STEP 5 – Transportation of Sample Vials: The pre-labelled sample vials are arranged in a tray and sent to the in-house pathology lab by General Duty Attendant (GDA) for analysis.
STEP 6 – Analysis of The Sample: The pathology technician receives the sample from the GDA on the prescribed form, do pre-analytical processing and finally process the samples in the automatic analysers one by one.
STEP 7 – Analysis Review – The processed samples are reviewed by the pathologist and final approval of the reports is done.
STEP 8 –Report Upload – The pathology technician uploads the approved reports on the HIS, which can be seen on the portal in the Critical Care Unit.
STEP 9 – Report Printing & Sorting – The nursing in-charge takes out the report prints and sort them to the respective patients.
STEP 10 – Report Information: The nursing staff looking for the patient informs the received report to the consultant on duty and note it down on the flow chart.
7. Application of Lean Principles
In the pre-analytical process described above, it was noted that there is UNEVENNESS, OVERBURDEN and WASTE – (Japanese Terms:
MURA MURI MUDA)
| [3] | Gupta, Rajiv, Session 6: Module 3: Understanding Waste, Lecture Notes, HHSM ZG615 Service Quality Excellence in Healthcare, BITS Pilani, delivered 17th Feb 2023. |
[3].
Mura/Unevenness: The exercise of routine blood sampling takes place at 5 am morning and approximately 20 samples are sent together to the lab. This policy of sampling and sending of blood samples in the early morning at 5 am is due to the following two reasons:
1) Pathology lab technician is free from the rush of OPD patients at the early morning hours.
2) The reports can be generated by 10 am, before the expected daily round of the treating consultant doctor.
Muri/Overburden: This peak of blood sampling and transportation of sample vials to the pathology lab goes on for around one hour in the early morning. This is identified as an overburden a potential cause of incorrect process or defects.
Muda/Waste: Such mistakes due to over burden are considered as a Waste Of Defect/Muda.
FIFO Logistics: It was further noted that by sending 20 samples in one batch, we are increasing the non-value-added time of the samples drawn first and processed last. The analysis of the samples also takes time. So, the time between the blood sample first drawn and analysed last might lead to erroneous results. To eliminate this waste, First In First Out (FIFO) Logistics were implemented.
7.1. Policy Change
1) The sampling, transportation of sample vials and analysis of samples (Step 4, 5 and 6) were made reiterative with lesser number of samples.
2) The samples are numbered according to the time sample withdrawn, so that the first sample gets processed first and reported first.
3) At around 4:30 am, samples of 4 to 5 patients are to be sent first, then second batch at 5 am, third at 5:30 am and fourth/last at 6 am.
4) Reporting also done in the same order, so that the printing and sorting of reports (Step 9 and 10) are also evened out.
Following advantages were immediately seen:
1) Easy supervision of small volume iterative process.
2) Reduction in wait time of blood samples getting processed.
3) Decrease in unevenness and burden on the healthcare personnel.
4) More clinical correlation of investigation reports. (subjectively)
Figure 3. Use of iterative process in small batch volumes to eliminate Mura, Muri & Muda. PDSA - an iterative process, to supervise and improve process.
7.2. Root Cause Analysis of Pre-Analytic Lab Errors
Since maximum errors are attributed to pre-analytic phase, specific problems need individual attention. For this purpose, Failure Modes and Effects Analysis (FMEA) is a proactive method and tool for detecting as well as prioritizing procedural errors.
FMEA was originally developed by the U.S. military in 1949 to proactively anticipate potential failures and became more widely used in the automotive industry in the 1970s. FMEA is already commonly used in hospital transfusion medicine and pharmacies but can be used to improve any process
.
FMEA was carried out for the pre-analytical phase of the lab investigation process and following potential modes were recognized after discussing the process in detail with the nursing staff, supervisors, medical officers and critical care consultants:
1) Inappropriate test request indentation
2) Labelling errors
3) Misidentification of patient
4) Inappropriate container
5) Improper sample collection technique
6) Inadequate sample/anticoagulant volume ratio
7) Inadequate mixing
8) Transportation & processing delay
Inappropriate test request indentation, labelling errors and misidentification of patient (nos. 1, 2 and 3) lead to wrong reports despite correct analysis. Whereas sampling errors (nos. 4, 5, 6 and 7) lead to erroneous sample causing wrong analysis despite correct analysis procedure. Transportation delays also lead to change in sample quality (eg. Hemolysis, cell clumping etc.) leading to wrong analysis.
For each failure mode, potential effects and consequences on the lab report as well as on the patient were listed in the prescribed FMEA process sheet (APPENDIX I). Each failure mode is ranked into three categories:
1) SEV - What is the severity of the error when it occurs?
2) OCC - What is the likelihood of occurrence?
3) DET - How difficult is it to detect the error?
Each category gets a score on a 1–10 scale (low to high), and the scores are multiplied together to give a risk priority number (RPN) for each failure mode. (
Table 3). The failure mode having highest RPN number is given the highest priority for initial attention and rectification
| [5] | Graban, Mark. (2016). Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement. CRC Press Taylor & Francis Group. |
[5]
. In our case,
improper sample collection technique was found to be having highest RPN number of 280, followed by inadequate sample volume (189) and improper mixing with anticoagulant (180). To control the process, a double check of steps is done either by the nursing in-charge or the resident medical officer.
Table 3. FMEA of Pre-Analytical process of laboratory testing.
Process Step | Potential Failure Mode | Potential Effect on Customer Because of Defect | SEV | Potential Causes | OCC | Current Process Controls | DET | RPN |
Test Order | Inappropriate test request indentation | Wrong Billing & Re-Testing; increased cost | 8 | Illegible Writing Reading error | 2 | Double check by Nursing In-charge | 2 | 32 |
Labelling | Labelling errors | Wrong report, increased cost | 8 | Random human error | 1 | Double check by supervisor | 1 | 8 |
Inappropriate container | Analysis error | 10 | Lack of training | 2 | Container selection by senior staff | 1 | 20 |
Sampling | Improper sample collection technique | Analysis error | 7 | Lack of training | 5 | Supervision by senior staff | 8 | 280 |
Inadequate sample/anticoagulant volume ratio | Analysis error | 9 | Lack of training Faulty equipment | 3 | Supervision by senior staff | 7 | 189 |
Inadequate mixing | Analysis error | 6 | Lack of training | 3 | Supervision by senior staff | 10 | 180 |
Transportation | Transportation & processing delay | Analysis error | 7 | Large volume Lack of staff | 2 | Noting turnaround time | 6 | 84 |
8. Control Measures
1) Removing fear – The nursing staff were assured of ‘no penal action’ due to sampling errors and were asked to enlist the problems faced during blood sampling process. The junior staff were prompted to report errors to correct the potential error zones and improve quality.
2) Double check – Sampling steps done by relatively less trained staff are supervised by senior staff or nursing in-charges. Indentation, container selection and labelling is always checked by nursing in-charge.
3) Training by senior staff – Nursing staff were given training sessions of proper single prick blood sampling technique, identifying problems during phlebotomy and various ways to troubleshoot them.
4) Reducing unevenness – Sampling blood of a smaller number of patients and distributing the process over longer period will make the process smooth and possibly error free.
5) Recording errors – Nursing supervisors and resident doctors were trained to make a record of both the active errors as well as latent errors detected in the process. For example, one staff member pointed out the inadequate supply of tourniquet for vein preparation. So inappropriate blood sampling was an active error and not applying tourniquet to prepare a vein was a latent error leading to active error.
6) Proper use of technology – Proper use of vacutainers, vial stands for transportation, bar coding for identification etc. were proposed as plans to improve quality of sampling for lab investigations.
7) Continuous evaluation and monitoring – Written schedules are made to re-evaluate the steps and monitor the incidence of errors. Regular monthly brainstorming sessions are planned to discuss the evaluation, monitoring and control measures.
9. Conclusion
Medical errors, including lab errors, are the most under reported patient safety issues in our country’s health care system. Besides compromising patient safety, they also increase the cost of treatment, decrease value vis a vis quality of services. The healthcare personnel fear disclosing the errors as it might further increase the gap of mistrust between public and our healthcare system. Senior management must take pro-active measures to eliminate this fear of error reporting and continuously standardize the process of lab testing, specially in an acute care setup. Acute care setups demonstrate a high volume of routine blood investigations, for which unevenness in the process often leads to overburden and mistakes. The processes should be re-programmed to make them as smooth and even as possible. Various studies have demonstrated that the pre-analytical phase of laboratory testing is the most vulnerable phase of errors. These processes should be continuously monitored, evaluated, and controlled by using process improvement tools like FMEA. Implementation of the principles of Lean Model should be integrated holistically by the organization to increase value and eliminate waste from the whole system. Making a system error free is not possible, but a near zero error system is a reality, often achieved by following the mentioned principles.
Abbreviations
NABL | National Accreditation Board for Testing and Calibration Laboratories |
ICU | Intensive Care Unit |
HDU | High Dependency Unit |
CBC | Complete Blood Count |
KFT | Kidney Function Tests |
GDA | General Duty Attendant |
HIS | Hospital Information System |
UHID No. | Unique Health Identification Number |
IPD No. | In-Patient Department Number |
OPD | Outpatient Department |
FMEA | Failure Modes and Effects Analysis |
FIFO | First In First Out |
RPN | Risk Priority Number |
Author Contributions
Muneel Abbas Rizvi: Conceptualization, Data curation, Writing - original draft
Zaibun Nisa: Formal Analysis, Investigation, Methodology, Project administration, Resources, Supervision
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Accreditation, Commission on Office Laboratory. n.d.
http://www.cola.org/
|
| [2] |
Halverson AL, Dintzis SM, Pavkovic S. 2016 Dec; "Surgical Specimen Management: A Descriptive Study of 648 Adverse Events and Near Misses." Arch Pathol Lab Med. 140(12): 1390-1396.
|
| [3] |
Gupta, Rajiv, Session 6: Module 3: Understanding Waste, Lecture Notes, HHSM ZG615 Service Quality Excellence in Healthcare, BITS Pilani, delivered 17th Feb 2023.
|
| [4] |
Institute for Healthcare Improvement, All FMEA Tools, AllTools.aspx (accessed August 9, 2015)
http://app.ihi.org/Workspace/tools/fmea/
|
| [5] |
Graban, Mark. (2016). Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement. CRC Press Taylor & Francis Group.
|
| [6] |
Womack, J. P., Jones, D. T., & Roos, D. (1990). The Machine That Changed the World: The Story of Lean Production. Free Press.
|
| [7] |
Shingo, S. (1986). Zero Quality Control: Source Inspection and the Poka-Yoke System. Productivity Press.
|
| [8] |
Radnor, Z., Holweg, M., & Waring, J. (2012). Lean in healthcare: The unfilled promise? Social Science & Medicine, 74(3), 364-371.
|
| [9] |
Rother, M., & Shook, J. (1999). Learning to See: Value Stream Mapping to Add Value and Eliminate MUDA. The Lean Enterprise Institute.
|
| [10] |
Kenney, C., & Florida, R. (2004). Locating Global Advantage: Industry Dynamics in the International Economy. Stanford University Press.
|
| [11] |
Toussaint, J. S., & Berry, L. L. (2013). The Promise of Lean in Health Care. Mayo Clinic Proceedings, 88(1), 74-82.
|
| [12] |
NHS Institute for Innovation and Improvement. (2007). The Lean Experience: A Story of Continuous Improvement.
|
| [13] |
Graban, M. (2012). Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement (2nd ed.). CRC Press.
|
| [14] |
Womack, J. P., & Jones, D. T. (2003). Lean Thinking: Banish Waste and Create Wealth in Your Corporation. Free Press.
|
| [15] |
Radnor, Z. J., Holweg, M., & Waring, J. (2012). Lean in healthcare: The unfilled promise? Social Science & Medicine, 74(3), 364-371.
|
Cite This Article
-
-
@article{10.11648/j.ajlm.20240905.11,
author = {Muneel Abbas Rizvi and Zaibun Nisa},
title = {Monitoring and Eliminating Pre-Analytic Laboratory Errors in an Acute Care Setup - A Case Study
},
journal = {American Journal of Laboratory Medicine},
volume = {9},
number = {5},
pages = {50-57},
doi = {10.11648/j.ajlm.20240905.11},
url = {https://doi.org/10.11648/j.ajlm.20240905.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20240905.11},
abstract = {Laboratory investigations are an integral part of patient management. The number and frequency of investigations are directly related to the clinical seriousness of a patient. Hence acute care setups observe a high volume as well as frequency of sampling for laboratory analyses. Many management plans are dependent on the results of these investigations. So, there is also pressure on the pathology laboratory to provide the results as early as possible. The whole process of lab investigation requires ordering an investigation, sending the requisition/system indenture, sampling, transporting sample to the lab, analysing, result approval and sending/uploading the report. Well-planned, tried, and tested standards/ protocols must be in place in order to eliminate the probability of errors in investigation reports. Laboratories must work according to some set specifications in order to process the samples in an error free manner. This paper will analyse the procedural steps, scope of errors and steps to identify, report as well as rectify the errors in the pre-analytical phase of laboratory investigations in a highly demanding and accident-prone acute care setup. The aim of this exercise is to improve the quality of lab reporting process with an objective to eliminate pre analytic laboratory errors.
},
year = {2024}
}
 Copy
|
Copy
|
 Download
Download
-
TY - JOUR
T1 - Monitoring and Eliminating Pre-Analytic Laboratory Errors in an Acute Care Setup - A Case Study
AU - Muneel Abbas Rizvi
AU - Zaibun Nisa
Y1 - 2024/11/29
PY - 2024
N1 - https://doi.org/10.11648/j.ajlm.20240905.11
DO - 10.11648/j.ajlm.20240905.11
T2 - American Journal of Laboratory Medicine
JF - American Journal of Laboratory Medicine
JO - American Journal of Laboratory Medicine
SP - 50
EP - 57
PB - Science Publishing Group
SN - 2575-386X
UR - https://doi.org/10.11648/j.ajlm.20240905.11
AB - Laboratory investigations are an integral part of patient management. The number and frequency of investigations are directly related to the clinical seriousness of a patient. Hence acute care setups observe a high volume as well as frequency of sampling for laboratory analyses. Many management plans are dependent on the results of these investigations. So, there is also pressure on the pathology laboratory to provide the results as early as possible. The whole process of lab investigation requires ordering an investigation, sending the requisition/system indenture, sampling, transporting sample to the lab, analysing, result approval and sending/uploading the report. Well-planned, tried, and tested standards/ protocols must be in place in order to eliminate the probability of errors in investigation reports. Laboratories must work according to some set specifications in order to process the samples in an error free manner. This paper will analyse the procedural steps, scope of errors and steps to identify, report as well as rectify the errors in the pre-analytical phase of laboratory investigations in a highly demanding and accident-prone acute care setup. The aim of this exercise is to improve the quality of lab reporting process with an objective to eliminate pre analytic laboratory errors.
VL - 9
IS - 5
ER -
Copy
|
Download