Feline herpesvirus type 1 (FHV-1) is a widespread pathogen responsible for feline viral rhinotracheitis, a highly contagious disease affecting cats worldwide. This virus primarily targets the upper respiratory tract and ocular tissues, leading to clinical signs such as sneezing, nasal discharge, conjunctivitis, keratitis, and, in severe cases, corneal ulceration. FHV-1 is particularly problematic in young, immunocompromised, or stressed cats, and latent infections can result in recurrent clinical manifestations. The pathogenesis of FHV-1 involves initial viral replication in epithelial cells, followed by latency establishment in the trigeminal ganglia. Reactivation can occur due to stress, immunosuppression, or co-infections, leading to viral shedding and disease recurrence. Diagnosis is based on clinical presentation, supported by molecular techniques such as PCR, which detect viral DNA in ocular or respiratory secretions. Serological tests are less useful due to widespread exposure among the feline population. Management of FHV-1 includes supportive care, antiviral therapy, and immune modulation. Topical and systemic antivirals, such as famciclovir and cidofovir, have shown efficacy in reducing viral replication and alleviating clinical symptoms. Interferon therapy and other immunomodulatory treatments are under investigation to enhance antiviral responses. Lysine supplementation, previously recommended, has shown conflicting results in recent studies. Secondary bacterial infections are common and may require antibiotic therapy. Vaccination plays a crucial role in prevention, though it does not completely eliminate the risk of infection or reactivation. Stress management and maintaining optimal environmental conditions can help reduce recurrence. Ocular complications of FHV-1, including chronic conjunctivitis, symblepharon, corneal sequestrum, and stromal keratitis, pose significant challenges in feline ophthalmology. Despite advances in diagnosis and treatment, FHV-1 remains a significant concern in feline medicine. Understanding its pathogenesis, improving management strategies, and developing more effective preventive measures are essential for minimizing its impact on feline health.
| Published in | American Journal of Laboratory Medicine (Volume 10, Issue 4) |
| DOI | 10.11648/j.ajlm.20251004.11 |
| Page(s) | 64-77 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Feline Herpesvirus (FHV-1), Feline Viral Rhinotracheitis, Feline Keratoconjunctivitis, Corneal Ulcers in Cats, Antiviral Therapy for Feline Herpes, FHV-1 Diagnosis and Treatment, Feline Herpesvirus Vaccine
FHV-1 | Feline Herpes Virus |
MDA | Maternal Derived Antibodies |
VNA | Virus Neutralizing Antibodies |
LAT | Latency-associated Transcript |
| [1] | Maggs D. J., Clarke H. E. "Relative sensitivity of polymerase chain reaction assays used for detection of feline herpesvirus type 1 DNA in clinical samples and commercial vaccines." American Journal of Veterinary Research, 2005, 60, 1550-1555. |
| [2] | Studdert M. J., Martin M. C. "Virus diseases of the respiratory tract of cats: 1. Isolation of feline rhinotracheitis virus." Australian Veterinary Journal, 1970, 46(3), 99-104. |
| [3] | Crotti A., Barsotti G. "Congiuntiviti, cheratiti e cheratocongiuntiviti infettive nel gatto Parte 2: herpesvirus felino." Veterinaria, 2024, 38(2). |
| [4] | Thomasy S. M., Maggs D. J. "A review of antiviral drugs and other compounds with activity against feline herpesvirus-1." Veterinary Ophthalmology, 2016, 19, 119-130. |
| [5] | Maes R. "Felid herpesvirus type 1 infection in cats: a natural host model for alphaherpesvirus pathogenesis." ISRN Veterinary Science, 2012, Article ID 495830. |
| [6] | Andrew S. E. "Ocular manifestations of feline herpesvirus." Journal of Feline Medicine and Surgery, 2001, 3, 9-16. |
| [7] | Monne Rodriguez J. M., Leeming G., Kohler K., Kipar A. "Feline herpesvirus pneumonia: investigations into the pathogenesis." Veterinary Pathology, 2017, 54(6), 922-932. |
| [8] | Rohowsky M. W., Griesemer R. A. "Experimental feline viral rhinotracheitis in the germfree cat." American Journal of Pathology, 1970, 58(2), 269-82. |
| [9] | Gaskell R., Dawson S., Radford A., Thiry E. "Feline herpesvirus." Veterinary Research, 2007, 38, 337-354. |
| [10] | Nasisse M. P., Guy J. S., Davidson M. G., Sussman W. A., Farley N. M. "Experimental ocular herpesvirus infection in the cat. Sites of virus replication, clinical features and effects of corticosteroid administration." Investigative Ophthalmology and Visual Science, 1989, 30(8), 1758-1768. |
| [11] | Stiles J. "Feline herpesvirus." Veterinary Clinics of North America: Small Animal Practice, 2000, 30(5), 1001-1014. |
| [12] | Maeda K., Horimoto T., Mikami T. "Properties and functions of feline herpesvirus type 1 glycoproteins." Journal of Veterinary Medical Science, 1998, 60(8), 881-888. |
| [13] | Deng M., Liang H., Xu Y., Shi Q., Bao F., Mei C., Dai Z., Huang X. "Identification, genetic characterization, and pathogenicity of three feline herpesvirus type 1 isolates from domestic cats in China." Veterinary Sciences, 2024, 11, 285. |
| [14] | Hamano M., Maeda K., Mizukoshi F., Une Y., Mochizuki M., Tohya Y., Akashi H., Kai K. "Experimental infection of recent field isolates of feline herpesvirus type 1." Journal of Veterinary Medical Science, 2003, 65(8), 939-943. |
| [15] | Sheldon Tai S. H., Niikura M., Cheng H. H., Kruger J. M., Wise A. G., Maes R. K. "Complete genomic sequence and an infectious BAC clone of feline herpesvirus-1 (FHV-1)." Virology, 2010, 401, 215-227. |
| [16] | Maggs D. J. "Update on pathogenesis, diagnosis and treatment of feline herpesvirus type 1." Clinical Techniques in Small Animal Practice, 2005, 20(2), 94-101. |
| [17] | Thiry E., Addie D., Belak S., Boucraut-Baralon C., Egberink H., Frymus T., et al. "Feline herpesvirus infection. ABCD guidelines on prevention and management." Journal of Feline Medicine and Surgery, 2009, 11, 547-555. |
| [18] | Hoover E. A. "Infectious disease of the dog and cat." In: Greene C. E. (Ed.), 4th Edition, Elsevier. |
| [19] | Lombardi R. "Persistent pupillary membranes in dogs and cats." Veterinaria, 2012, 2, 97-104. |
| [20] | Gaskell R. M., Povey R. C. "Experimental induction of feline viral rhinotracheitis virus re-excretion in FVR-recovered cats." The Veterinary Record, 1977, 12, 128-133. |
| [21] | Gaskell R. M., Povey R. C., Transmission of feline viral rhinotracheitis. Vet Rec. 1982; 111: 359-362. |
| [22] | Synowiec A., Dąbrowka A., Pachota M., Baouche M., Owczarek K., Niżański W., Pyrc K., Feline herpesvirus 1 (FHV-1) enters the cell by receptor-mediated endocytosis. J Virol. 2023; 97(8): e00117-23. |
| [23] | Labin B. A., Chigbu D. I., Clinical management of herpes simplex virus keratitis. Diagnostics. 2022; 12(8): 2368. |
| [24] | Dunn L. E., Birkenheuer C. H., Dufour R., Baines J. D., Immediate early proteins of herpes simplex virus transiently repress viral transcription before subsequent activation. J Virol. 2022; 96(22): e01222-22. |
| [25] | Townsend W. M., Stiles J., Guptill-Yoran L., Krohne S. G., Development of a reverse transcriptase-polymerase chain reaction assay to detect feline herpesvirus-1 latency-associated transcripts in the trigeminal ganglia and corneas of cats that did not have clinical signs of ocular disease. Am J Vet Res. 2004; 65(3): 314-319. |
| [26] | Wang Q., Zhou C., Johnson K., Colgrove R. C., Coen D. M., Knipe D. M., Herpesviral latency-associated transcript gene promotes assembly of heterochromatin on viral lytic-gene promoters in latent infection. Proc Natl Acad Sci U S A. 2005; 102(44): 16055-16059. |
| [27] | Kennedy D. P., Clement C., Arceneaux R. L., Bhattacharjee P. S., Huq T. S., Hill J. M., Ocular HSV-1: is the cornea a reservoir for viral latency or a fast pit stop? Cornea. 2011; 30(3): 251-257. |
| [28] | Jones C., Alphaherpesvirus latency: its role in disease and survival of the virus in nature. Adv Virus Res. 1998; 51: 81-133. |
| [29] | Nasisse M. P., Glover T. L., Moore C. P., Detection of feline herpesvirus 1 DNA in corneas of cats with eosinophilic keratitis or corneal sequestrum. Am J Vet Res. 1998; 59(7): 856-858. |
| [30] | Stiles J., McDermott B. S., Bigsby D., Willis M., Martin C., Roberts W., Use of nested polymerase chain reaction to identify feline herpesvirus in ocular tissue from clinically normal cats and cats with corneal sequestra or conjunctivitis. Am J Vet Res. 1997; 58(4): 338-342. |
| [31] | Maggs D. J., Lappin M. R., Nasisse M. P., Detection of feline herpesvirus-specific antibodies and DNA in aqueous humor from cats with or without uveitis. Am J Vet Res. 1999; 60(8): 932-936. |
| [32] | Liesegang T. J., Classification of herpes simplex virus keratitis and anterior uveitis. Cornea. 1999; 18(2): 127-143. |
| [33] | Hargis A. M., Ginn P. E., Feline herpesvirus 1 associated facial and nasal dermatitis and stomatitis in domestic cats. Vet Clin North Am Small Anim Pract. 1999; 29(6): 1281-1290. |
| [34] | Malik R., Lessels N. S., Webb S., Gotis-Graham P., Vitale C., Norris J. M., Power H., Treatment of feline herpesvirus-1 associated disease in cats with famciclovir and related drugs. J Feline Med Surg. 2009; 11(1): 40-48. |
| [35] | Johnson L. R., Foley J. E., De Cock H. V., Clarke H. E., Maggs D. J., Assessment of infectious organisms associated with chronic rhinosinusitis in cats. J Am Vet Med Assoc. 2005; 227(4): 579-585. |
| [36] | Hartley C., Aetiology of corneal ulcers. Assume FHV-1 unless proven otherwise. J Feline Med Surg. 2010; 12(1): 24-35. |
| [37] | Gould D., Feline herpesvirus-1: ocular manifestations, diagnosis and treatment options. J Feline Med Surg. 2011; 13(5): 333-346. |
| [38] | Stiles J., Treatment of cats with ocular disease attributable to herpesvirus infection: 17 cases (1983-1993). J Am Vet Med Assoc. 1995; 207(5): 599-603. |
| [39] | Low H. C., Powell C. C., Veir J. K., Hawley J. R., Lappin M. R., "Prevalence of feline Herpesvirus 1, Chlamydophila felis, and mycoplasma spp DNA in conjunctival cells collected from cats with and without conjunctivitis." American Journal of Veterinary Research, 2007, vol. 68, no. 6, pp. 643-648. |
| [40] | Hartmann A. D., Hawley J., Werckenthin C., Lappin M. R., Hartmann K., "Detection of bacterial and viral organisms from the conjunctiva of cats with conjunctivitis and upper respiratory tract disease." Journal of Feline Medicine and Surgery, 2010, vol. 12, pp. 775-780. |
| [41] | Nasisse M. P., Guy J. S., Stevens J. B., English R. V., Davidson G., "Clinical and laboratory findings in chronic conjunctivitis in cats: 91 cases (1983-1991)." Journal of the American Veterinary Medical Association, 1993, vol. 203, no. 6, pp. 834-840. |
| [42] | Dean E., Meunier V., "Feline eosinophilic keratoconjunctivitis: a retrospective study of 45 cases (56 eyes)." Journal of Feline Medicine and Surgery, 2013, vol. 15, no. 8, pp. 661-666. |
| [43] | Prasse K. W., Winston S. M., "Cytology and histopathology of feline eosinophilic keratitis." Veterinary and Comparative Ophthalmology, 1996, vol. 6, no. 2, pp. 74-81. |
| [44] | Stiles J., "Treatment of cats with ocular disease attributable to herpesvirus infection: 17 cases (1983-1993)." Journal of the American Veterinary Medical Association, 1995, vol. 207, no. 5, pp. 599-603. |
| [45] | Chan N. S. W., Chee S. P., "Demystifying viral anterior uveitis: A review." Clinical and Experimental Ophthalmology, 2019, vol. 47, no. 3, pp. 320-333. |
| [46] | Doymaz M. Z., Rouse B. T., "Immunopathology of herpes simplex virus infections." Current Topics in Microbiology and Immunology, 1992, vol. 179, pp. 121-136. |
| [47] | Lim C. C., Reilly C. M., Thomasy S. M., Kass P. H., Maggs D. J., "Effects of feline herpesvirus type 1 on tear film break-up time, Schirmer tear test results, and conjunctival goblet cell density in experimentally infected cats." American Journal of Veterinary Research, 2009, vol. 70, no. 3, pp. 394-403. |
| [48] | Sebbag L., Thomasy S. M., Leland A., Mukai M., Kim S., Maggs D. J., "Altered corneal innervation and ocular surface homeostasis in FHV-1-exposed cats: a preliminary study suggesting metaherpetic disease." Frontiers in Veterinary Science, 2021, vol. 7, article 1. |
| [49] | Dawson E., Gaskell R. M., "Inconvenienti legati alla vaccinazione contro le infezioni respiratorie virali nel gatto." Veterinaria, 1995, anno 9, no. 1, pp. 105-109. |
| [50] | Stiles J., Pogranichniy R., "Detection of virulent herpesvirus-1 in the corneas of clinically normal cats." Journal of Feline Medicine and Surgery, 2008, vol. 10, pp. 154-159. |
| [51] | Green M. R., Sambrook J., "Nested polymerase chain reaction (PCR)." Cold Spring Harbor Protocols, 2019, vol. 2019, no. 1, pp. 175-178. |
| [52] | Vögtlin A. C., Fraefel C., Albini S., Leutenegger C. M., Schraner E., Spiess B., Lutz H., Ackermann M., "Quantification of feline herpesvirus 1 DNA in ocular fluid samples of clinically diseased cats by real-time TaqMan PCR." Journal of Clinical Microbiology, 2002, vol. 40, no. 2, pp. 519-523. |
| [53] | Goldschmidt P., Rostane H., Saint-Jean C., Batellier L., Alouch C., Zito E., Bourcier T., Laroche L., Chaumeil C., "Effects of topical anaesthetics and fluorescein on the real-time PCR used for the diagnosis of Herpesviruses and Acanthamoeba keratitis." British Journal of Ophthalmology, 2006, vol. 90, no. 11, pp. 1354-1356. |
| [54] | Maggs D. J., "Antiviral therapy for feline herpesvirus infections." Veterinary Clinics of North America: Small Animal Practice, 2010, vol. 40, no. 6, pp. 1055-1062. |
| [55] | Fontanelle J. P., Powell C. C., Veir J. K., Radecki S. V., Lappin M. R., "Effect of topical ophthalmic application of cidofovir on experimentally induced primary ocular feline herpesvirus-1 infection in cats" American Journal of Veterinary Research, 2008, 69, 289-293. |
| [56] | Williams D. L., Robinson J. C., Lay E., Field H., "Efficacy of topical acyclovir for the treatment of feline herpetic keratitis: results of a prospective clinical trial and data from in vitro investigations" Veterinary Record, 2005, 157, 254-257. |
| [57] | Thomasy S. M., Lim C. C., Reilly C. M., Kass P. H., Lappin M. R., Maggs D. J., "Evaluation of orally administered famciclovir in cats experimentally infected with feline herpesvirus type-1" American Journal of Veterinary Research, 2011, 72, 85-95. |
| [58] | Maggs D. J., Collins B. K., Thorne J. G., Nasisse M. P., "Effects of L-lysine and L-arginine on in vitro replication of feline herpesvirus type-1" American Journal of Veterinary Research, 2000, 61, 1474-1478. |
| [59] | Stiles J., Townsend W. M., Roger Q. R., Krohne S. G., "Effect of oral administration of L-lysine on conjunctivitis caused by feline herpesvirus in cats" American Journal of Veterinary Research, 2002, 63, 99-103. |
| [60] | Maggs D. J., Nasisse M. P., Kass P. H., "Efficacy of oral supplementation with L-lysine in cats latently infected with feline herpesvirus" American Journal of Veterinary Research, 2003, 64, 37-42. |
| [61] | Drazenovich T. L., Fascetti A. J., Westermeyer H. D., Sykes J. E., Bannasch M. J., Kass P. H., Hurley K. F., Maggs D. J., "Effects of dietary lysine supplementation on upper respiratory and ocular disease and detection of infectious organisms in cats within an animal shelter" American Journal of Veterinary Research, 2009, 70, 1391-1400. |
| [62] | Rees T. M., Lubinski J. L., "Oral supplementation with L-lysine did not prevent upper respiratory infection in a shelter population of cats" Journal of Feline Medicine and Surgery, 2008, 10, 510-513. |
| [63] | Maggs D. J., Sykes J. E., Clarke H. E., Yoo S. H., Kass P. H., Lappin M. R., Roger Q. R., Waldron M. K., Fascetti A. J., "Effects of dietary lysine supplementation in cats with enzootic upper respiratory disease" Journal of Feline Medicine and Surgery, 2007, 9, 97-108. |
| [64] | Haid C., Kaps S., Gonczi E., Hassig M., Metzler A., Spiess B., Richter M., "Pretreatment with feline interferon omega and the course of subsequent infection with feline herpesvirus in cats" Veterinary Ophthalmology, 2007, 10(5), 278-284. |
| [65] | Slack J., Stiles J., Leutenegger C. M., Moore G., Pogranichniy R. M., "Effects of topical ocular administration of high doses of human recombinant interferon alpha-2b and feline recombinant interferon omega on naturally occurring viral keratoconjunctivitis in cats" American Journal of Veterinary Research, 2013, 74, 281-289. |
| [66] | Fulton R. W., Burge L. J., "Susceptibility of feline herpesvirus 1 and a feline calicivirus to feline interferon and recombinant human leukocyte interferons" Antimicrobial Agents and Chemotherapy, 1985, 28(5), 698-699. |
| [67] | Bracklein T., Theise S., Metzler A., Spiess B. M., Richter M., "Activity of feline interferon-omega after ocular or oral administration in cats as indicated by Mx protein expression in conjunctival and white blood cells" American Journal of Veterinary Research, 2006, 67(6), 1025-1032. |
| [68] | Nasisse M. P., English R. V., Tompkins M. B., Guy J. S., Sussman W. A., "Immunologic, histologic, and virologic features of herpesvirus-induced stromal keratitis in cats" American Journal of Veterinary Research, 1995, 56(1), 51-55. |
| [69] | Tanaka A., Wagner D. C., Kass P. H., Hurley K. F., "Association among weight loss, stress, and upper respiratory tract infection in shelter cats." Journal of the American Veterinary Medical Association, 2012, vol. 240, no. 5, pp. 570-576. |
| [70] | Worranan K., Jarudecha T., Rattanatumhi K., Ritchoo S., Muikaew R., Wangsud S., Sussadee M., "First study on stress evaluation and reduction in hospitalized cats after neutering surgery." Veterinary World, 2022, vol. 15, pp. 1-8. |
| [71] | Gourkow N., Phillips C. J. C., "Effect of interaction with humans on behaviour, mucosal immunity and upper respiratory disease of shelter cats rated as contented on arrival." Preventive Veterinary Medicine, 2015, vol. 121, pp. 288-296. |
| [72] | Contreras E. T., Hodgkins E., Tynes V., Beck A., Olea-Popelka F., Lappin M. R., "Effect of a pheromone on stress-associated reactivation of feline herpesvirus-1 in experimentally inoculated kittens." Journal of Veterinary Internal Medicine, 2018, vol. 32, pp. 406-417. |
| [73] | M. A. Mironovich 1, A. Yoon, M. E Marino 1, N. E. Ineck, i Liu 1, R. T Carter 1, A. C Lewin 1 “Evaluation of compounded cidofovir, famciclovir, and ganciclovir for the treatment of feline herpesvirus ocular surface disease in shelter-housed cats” Vet Ophthalmol 2023 Apr: 26 Suppl 1: 143-153. |
APA Style
Lombardi, R. (2025). Feline Herpesvirus: A Persistently Relevant Disease, from Infection to Clinical Management. American Journal of Laboratory Medicine, 10(4), 64-77. https://doi.org/10.11648/j.ajlm.20251004.11
ACS Style
Lombardi, R. Feline Herpesvirus: A Persistently Relevant Disease, from Infection to Clinical Management. Am. J. Lab. Med. 2025, 10(4), 64-77. doi: 10.11648/j.ajlm.20251004.11
@article{10.11648/j.ajlm.20251004.11,
author = {Roberto Lombardi},
title = {Feline Herpesvirus: A Persistently Relevant Disease, from Infection to Clinical Management
},
journal = {American Journal of Laboratory Medicine},
volume = {10},
number = {4},
pages = {64-77},
doi = {10.11648/j.ajlm.20251004.11},
url = {https://doi.org/10.11648/j.ajlm.20251004.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20251004.11},
abstract = {Feline herpesvirus type 1 (FHV-1) is a widespread pathogen responsible for feline viral rhinotracheitis, a highly contagious disease affecting cats worldwide. This virus primarily targets the upper respiratory tract and ocular tissues, leading to clinical signs such as sneezing, nasal discharge, conjunctivitis, keratitis, and, in severe cases, corneal ulceration. FHV-1 is particularly problematic in young, immunocompromised, or stressed cats, and latent infections can result in recurrent clinical manifestations. The pathogenesis of FHV-1 involves initial viral replication in epithelial cells, followed by latency establishment in the trigeminal ganglia. Reactivation can occur due to stress, immunosuppression, or co-infections, leading to viral shedding and disease recurrence. Diagnosis is based on clinical presentation, supported by molecular techniques such as PCR, which detect viral DNA in ocular or respiratory secretions. Serological tests are less useful due to widespread exposure among the feline population. Management of FHV-1 includes supportive care, antiviral therapy, and immune modulation. Topical and systemic antivirals, such as famciclovir and cidofovir, have shown efficacy in reducing viral replication and alleviating clinical symptoms. Interferon therapy and other immunomodulatory treatments are under investigation to enhance antiviral responses. Lysine supplementation, previously recommended, has shown conflicting results in recent studies. Secondary bacterial infections are common and may require antibiotic therapy. Vaccination plays a crucial role in prevention, though it does not completely eliminate the risk of infection or reactivation. Stress management and maintaining optimal environmental conditions can help reduce recurrence. Ocular complications of FHV-1, including chronic conjunctivitis, symblepharon, corneal sequestrum, and stromal keratitis, pose significant challenges in feline ophthalmology. Despite advances in diagnosis and treatment, FHV-1 remains a significant concern in feline medicine. Understanding its pathogenesis, improving management strategies, and developing more effective preventive measures are essential for minimizing its impact on feline health.
},
year = {2025}
}
TY - JOUR T1 - Feline Herpesvirus: A Persistently Relevant Disease, from Infection to Clinical Management AU - Roberto Lombardi Y1 - 2025/09/15 PY - 2025 N1 - https://doi.org/10.11648/j.ajlm.20251004.11 DO - 10.11648/j.ajlm.20251004.11 T2 - American Journal of Laboratory Medicine JF - American Journal of Laboratory Medicine JO - American Journal of Laboratory Medicine SP - 64 EP - 77 PB - Science Publishing Group SN - 2575-386X UR - https://doi.org/10.11648/j.ajlm.20251004.11 AB - Feline herpesvirus type 1 (FHV-1) is a widespread pathogen responsible for feline viral rhinotracheitis, a highly contagious disease affecting cats worldwide. This virus primarily targets the upper respiratory tract and ocular tissues, leading to clinical signs such as sneezing, nasal discharge, conjunctivitis, keratitis, and, in severe cases, corneal ulceration. FHV-1 is particularly problematic in young, immunocompromised, or stressed cats, and latent infections can result in recurrent clinical manifestations. The pathogenesis of FHV-1 involves initial viral replication in epithelial cells, followed by latency establishment in the trigeminal ganglia. Reactivation can occur due to stress, immunosuppression, or co-infections, leading to viral shedding and disease recurrence. Diagnosis is based on clinical presentation, supported by molecular techniques such as PCR, which detect viral DNA in ocular or respiratory secretions. Serological tests are less useful due to widespread exposure among the feline population. Management of FHV-1 includes supportive care, antiviral therapy, and immune modulation. Topical and systemic antivirals, such as famciclovir and cidofovir, have shown efficacy in reducing viral replication and alleviating clinical symptoms. Interferon therapy and other immunomodulatory treatments are under investigation to enhance antiviral responses. Lysine supplementation, previously recommended, has shown conflicting results in recent studies. Secondary bacterial infections are common and may require antibiotic therapy. Vaccination plays a crucial role in prevention, though it does not completely eliminate the risk of infection or reactivation. Stress management and maintaining optimal environmental conditions can help reduce recurrence. Ocular complications of FHV-1, including chronic conjunctivitis, symblepharon, corneal sequestrum, and stromal keratitis, pose significant challenges in feline ophthalmology. Despite advances in diagnosis and treatment, FHV-1 remains a significant concern in feline medicine. Understanding its pathogenesis, improving management strategies, and developing more effective preventive measures are essential for minimizing its impact on feline health. VL - 10 IS - 4 ER -
Clinica Veterinaria Giaconella, Roma, Italy
Figure 1. Taxonomy of Feline Herpesvirus 1 (FHV-1).

Figure 2. Facial dermatitis in a cat. (Courtesy of Dr. Necci F.).
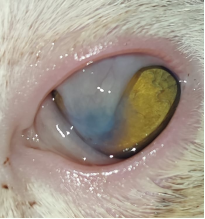
Figure 3. Symblepharon. (Courtesy of Dr. Naso S.).
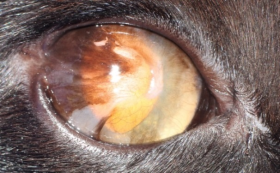
Figure 4. Lateral canthus symblepharon. Note the corneal neovascularization (chronic stromal keratitis). (Courtesy of Dr. Perez T.).
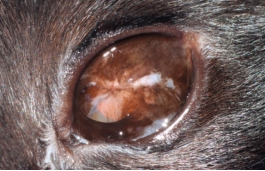
Figure 5. Pigmented symblepharon. (Courtesy of Dr. Perez T.).
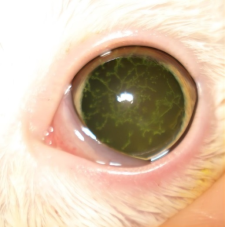
Figure 6. Dendritic corneal ulcer positive to fluorescein stain. (Courtesy of Dr. Tralhao P.).
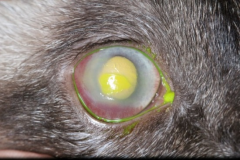
Figure 7. Chronic geographic ulcer. The ulcer is positive to fluorescein stain, with intense neovascularization and edema.
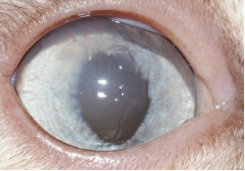
Figure 8. Geographic corneal ulcer without fluorescein stain. Note the central edema.
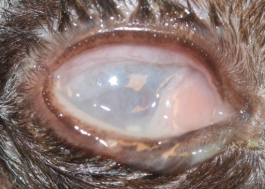
Figure 9. Acute herpes infection in a kitten. Conjunctivitis with purulent discharge.
Figure 10. Synopsis of the management of infected subjects.
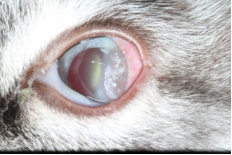
Figure 11. Eosinophilic keratitis. Note the white plaques. (Courtesy of Dr. Tralhao P.).

Figure 12. Corneal sequestrum in a cat. (Courtesy of Dr. Tralhao P.).

Figure 13. Corneal sequestrum. (Courtesy of Dr. Tralhao P.).
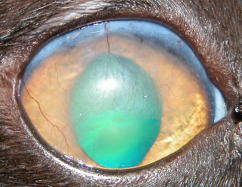
Figure 14. Chronic stromal keratitis in a cat. Note the intense fibrosis and neovascularization. (Courtesy of Dr. Vergara M.).

Figure 15. Chronic stromal keratitis.

