Thrombocytopenia is defined as a platelet count of less than 150 G/L in the blood. It can be of central or peripheral origin. Newly-formed immature platelets are called reticulated platelets (RP) and are expressed as the immature platelet fraction or IPF. This automated hematological parameter enables us to distinguish between peripheral and central thrombocytopenia in a simple, quick, easily reproducible and non-invasive way. In the present study, our aim was to evaluate the clinical utility of the IPF and its ability to differentiate between central and peripheral thrombocytopenia. In this prospective study, we collected 50 cases of thrombocytopenia in our series. The IPF and all other CBC parameters were measured using the Sysmex XN-1500 analyser. Based on the clinical context and myelogram findings, the subjects in our study were separated into a central thrombocytopenia group and a peripheral thrombocytopenia group. We then assessed variations in IPF between the two groups. The mean IPF in the peripheral thrombocytopenia group was significantly higher than that in the central thrombocytopenia group (15.71 ± 12.02% vs. 5.51 ± 3.04%; p<0.001) and this difference persisted regardless of platelet count. We also established a sensitivity and specificity ROC curve, which showed that the IPF had excellent diagnostic value for differentiating between central and peripheral thrombocytopenia, with an area under the curve of 0.914. We also defined a discriminative cut-off value of 8.5% with a sensitivity of 77.8% and a specificity of 86.4% for defining the origin of thrombocytopenia. Thus, an IPF value above 8.5% points to peripheral thrombocytopenia with increased platelet regeneration. In conclusion, the results of our study have enabled us to formulate recommendations for improving the diagnostic strategy for thrombocytopenia using the immature platelet fraction or IPF.
| Published in | American Journal of Laboratory Medicine (Volume 9, Issue 1) |
| DOI | 10.11648/j.ajlm.20240901.11 |
| Page(s) | 1-7 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Immatures Platelets, Peripheral Thrombocytopenia, Central Thrombocytopenia, Reticulated Platelets, Fluoro-Flowcytometry
2.1. Patients
2.1.1. Control Group
2.1.2. Thrombocytopenic Patients
2.2. Methods
2.2.1. Data Collection
2.2.2. Diagnostic Resources
3.1. Control Group
3.2. Thrombocytopenic Group
Patients | |
|---|---|
Nombre de patients | 50 (100%) |
Age | 54 (18-90) |
Males | 30 (60%) |
Cytopenias | |
Thrombocytopenia alone | 21 (42%) |
+ Anemia | 18 (36%) |
+ Neutropenia | 2 (4%) |
Pancytopenia | 9 (18%) |
Mechanism | |
Peripheral thrombocytopenia | 28 (56%) |
Consumption | 8 (16%) |
Hemorrhage/thrombosis | 2 (4%) |
Thrombotic micro-angiopathy | 4 (8%) |
Inflammation | 2 (4%) |
Hypersplenism | 1 (2%) |
Destruction | 19 (38%) |
Immune thrombocytopenia | 18 (36%) |
Evans syndrome | 1 (2%) |
Central thrombocytopenia | 22 (44%) |
Acute Leukaemia | 11 (22%) |
Myelodysplastic syndrome | 5 (10%) |
Bone metastasis | 3 (6%) |
Macrophage activation syndrome | 1 (1%) |
Primary myelofibrosis | 1 (2%) |
Drug toxicity (heparin treatment) | 1 (2%) |
Platelet count, G/L | |
Overall | 57,2 [1–100] |
PT | 54 [1–100] |
CT | 59 [5–84] |
IPF, % | |
Overall | 11,77 [1,1–67.3] |
PT | 15.71 [5.9–67.3] |
CT | 5.51 [1,1–18.5] |
Cut-off value | Sensitivity | Specificity | PPV | NPV | Youden’s Index | ASC |
|---|---|---|---|---|---|---|
8,5% | 77,8% | 86,4% | 97,25% | 77,14% | 0,641 | 0.914 |
1st author | Year of publication | Population | N | Sysmex instrument | % IPF |
|---|---|---|---|---|---|
Ali U [7 ] | 2017 | UK | 2292 | XN 1000 | 1.6–10.1 |
Yang B [8 ] | 2017 | China | 2179 | XN 9000 | 0.7–8.4 |
Ko YJ [9 ] | 2014 | Korea | 2104 | XE 2100/XN | 0.3–7.4 |
Mogongoa LF [10 ] | 2012 | South Africa | 60 | XE 2100 | 0.7–5.5 |
Sachdev R [11 ] | 2014 | India | 945 | XE 2100 | 0.3–8.7 |
Jung H [12 ] | 2012 | Korea | 2039 | XE 2100 | 0.4–3.2 |
Joergensen MK [13 ] | 2016 | Denmark | 1674 | XE 5000 | 1.3–9 |
Naz A [14 ] | 2016 | Pakistan | 94 | XE 2100 | 1.1–17.8 |
Cybulska A [15 ] | 2016 | Germany | 97 | XE 2100 | 0.9–8.5 |
Morkis IVC [16 ] | 2016 | Brazil | 132 | XE 5000 | 0.8–6.1 |
Our study | 2023 | Morocco | 100 | XN 1500 | 0.7-9.6 |
IPF% cut-off | Sensibility (%) | Specificity (%) | |
|---|---|---|---|
Jung et Al 2010, Korea [12 ] | 7,3 | 54 | 92,2 |
Abe et Al 2006, Japan [1 8] | 7,7 | 86,8 | 92,6 |
Asghar et Al 2023, Pakistan [22 ] | 7,95 | 92 | 86 |
Goel et Al 2021, India [23 ] | 5,95 | 88 | 75,9 |
Cho YG [24 ] | 6,1 | 92,9 | 82,9 |
Min Ji Jeon [2 1] | 7 | 61 | 70 |
Our study | 8,5 | 77,8 | 86,4 |
| [1] | Z. Van De Wyngaert, et al., Immature platelet fraction (IPF): A reliable tool to predict peripheral thrombocytopenia, Curr Res Transl Med (2019), |
| [2] | Benlachgar N, Doghmi K, Masrar A, Mahtat EM, Harmouche H, Tazi Mezalek Z. Immature platelets: a review of the available evidence. Thrombosis Research. 1 Novembre 2020; 195: 43‑50. |
| [3] | J. J. M. L. Hoffmann, Reticulated platelets: analytical aspects and clinical utility, Clin Chem Lab Med. 52(8) (2014) 1107–1117 août. |
| [4] | M. Nishiyama, S. Hayashi, O. Kabutomori, H. Yamanishi, E. Suehisa, Y. Kurata, et al., Effects of anticoagulants and storage temperature on immature platelet fraction % (IPF%) values in stored samples measured by the automated hematology analyzer, Rinsho Byori 59(5) (2011) 452–458 mai. |
| [5] | Ingram M, Coopersmith S. Reticulated platelets following acute blood loss. Br J Haematol 1969; 17: 225 – 8. |
| [6] | Koh KR, Yamane T, Ohta K, Hino M, Takubo T, Tatsumi N. Pathophysiological significance of simultaneous measurement of reticulated platelets, large platelets and serum thrombopoietin in non-neoplastic thrombocytopenic disorders. Eur J Haematol 1999; 63: 295 – 301. |
| [7] | U. Ali, G. Knight, R. Gibbs, D. A. Tsitsikas, Reference intervals for absolute and percentage immature platelet fraction using the Sysmex XN-10 automated haematology analyser in a UK population, Scand J Clin Lab Invest. 77(8) (2017) 658–664 déc. |
| [8] | B. Yang, Y. Zhou, S. Ding, H. Zha, F. Zhang, W. He, Y. Xu, Establishment of reference interval for immature platelet fraction using Sysmex XN9000 hematology analyzer in Anhui province in China, Int J Clin Exp Med 10(2017) 4214–4220. |
| [9] | Y. J. Ko, H. Kim, M. Hur, S. G. Choi, H.-W. Moon, Y.-M. Yun, et al., Establishment of reference interval for immature platelet fraction, Int J Lab Hematol. 35(5) (2013) 528–533 oct. |
| [10] | L. F. Mogongoa, J. Botma, A. D. Jaftha, W. J. van Rensburg, Reference ranges for platelet indices using Sysmex XE-2100 blood analyser, Med Technol SA 26(2012) 17–21. |
| [11] | R. Sachdev, A. K. Tiwari, S. Goel, V. Raina, M. Sethi, Establishing biological reference intervals for novel platelet parameters (immature platelet fraction, high immature platelet fraction, platelet distribution width, platelet large cell ratio, platelet-X, plateletcrit, and platelet distribution width) and their correlations among each other, Indian J Pathol Microbiol. 57(2) (2014) 231–235 juin. |
| [12] | H. Jung, H.-K. Jeon, H.-J. Kim, S.-H. Kim, Immature platelet fraction: establishment of a reference interval and diagnostic measure for thrombocytopenia, Korean J Lab Med. 30(5) (2010) 451–459 oct. |
| [13] | M. K. Joergensen, L. Bathum, Reference intervals for mean platelet volume and immature platelet fraction determined on a sysmex XE5000 hematology analyzer, Scand J Clin Lab Invest. 76(2) (2016) 172–176. |
| [14] | A. Naz, S. N. Mukry, M. R. Shaikh, A. R. Bukhari, T. S. Shamsi, Importance of immature platelet fraction as predictor of immune thrombocytopenic purpura, Pak J Med Sci. 32(3) (2016) 575–579 juin. |
| [15] | A. Cybulska, L. Meintker, J. Ringwald, S. W. Krause, Measurements of immature platelets with haematology analysers are of limited value to separate immune thrombocytopenia from bone marrow failure, Br J Haematol. 177(4) (2017) 612–619 mai. |
| [16] | I. V. C. Morkis, M. G. Farias, L. Scotti, Determination of reference ranges for immature platelet and reticulocyte fractions and reticulocyte hemoglobin equivalent, Rev Bras Hematol E Hemoter. 38(4) (2016) 310–313 déc. |
| [17] | Cannavo I, Ferrero-Vacher C, Sudaka I, Aquaronne D, Berthier F, Raynaud S. [Assessment of an immature platelet fraction (IFP%) in the diagnosis of thrombocytopenia]. Ann Biol Clin (Paris). |
| [18] | Abe Y, Wada H, Tomatsu H, Sakaguchi A, Nishioka J, Yabu Y, et al. A simple technique to determine thrombopoiesis level using immature platelet fraction (IPF). Thromb Res. 2006; 118(4): 463-9. |
| [19] | Ferreira FLB, Colella MP, Medina SS, Costa-Lima C, Fiusa MML, Costa LNG, et al. Evaluation of the immature platelet fraction contribute to the differential diagnosis of hereditary, immune and other acquired thrombocytopenias. Sci Rep 2017; 7(1): 3355. |
| [20] | Adly AA, Ragab IA, Ismail EA, et al. Evaluation of the immature platelet fraction in the diagnosis and prognosis of childhood immune thrombocytopenia. Platelets 2015; 26: 645–50. |
| [21] | Min Ji Jeon et al. Immature platelet fraction based diagnostic predictive scoring model for immune thrombocytopenia, Korean J Intern Med 2020; 35: 970-978. |
| [22] | Asghar MB, Akhtar F, Mahmood A, Rafique N, Rana NA, Khalid UB. Diagnostic Accuracy of Immature Platelet Fraction (IPF) to Differentiate Between Thrombocytopenia due to Peripheral Destruction versus Bone Marrow Failure. J Coll Physicians Surg Pak. Juillet 2023; 33(7): 760‑4. |
| [23] | Goel G, Semwal S, Khare A, Joshi D, Amerneni CK, Pakhare A, et al. Immature Platelet Fraction: Its Clinical Utility in Thrombocytopenia Patients. J Lab Physicians. Septembre 2021; 13(3): 214‑8. |
| [24] | Y. G. Cho, J. H. Lee, D. S. Kim, H. S. Lee, S. I. Choi, Clinical usefulness of the simple technique to diagnose thrombocytopenia using immature platelet fraction, Korean J Lab Med. 27(1) (2007) 1–6 févr. |
APA Style
Meskini, M. A., Bazi, K. E., Yahyaoui, H., Ameur, M. A., Chakour, M. (2024). Importance of the Immature Platelet Fraction in the Etiological Diagnosis of Thrombocytopenia. American Journal of Laboratory Medicine, 9(1), 1-7. https://doi.org/10.11648/j.ajlm.20240901.11
ACS Style
Meskini, M. A.; Bazi, K. E.; Yahyaoui, H.; Ameur, M. A.; Chakour, M. Importance of the Immature Platelet Fraction in the Etiological Diagnosis of Thrombocytopenia. Am. J. Lab. Med. 2024, 9(1), 1-7. doi: 10.11648/j.ajlm.20240901.11
AMA Style
Meskini MA, Bazi KE, Yahyaoui H, Ameur MA, Chakour M. Importance of the Immature Platelet Fraction in the Etiological Diagnosis of Thrombocytopenia. Am J Lab Med. 2024;9(1):1-7. doi: 10.11648/j.ajlm.20240901.11
@article{10.11648/j.ajlm.20240901.11,
author = {Mohammed Ali Meskini and Kenza El Bazi and Hicham Yahyaoui and Mohamed Ait Ameur and Mohamed Chakour},
title = {Importance of the Immature Platelet Fraction in the Etiological Diagnosis of Thrombocytopenia
},
journal = {American Journal of Laboratory Medicine},
volume = {9},
number = {1},
pages = {1-7},
doi = {10.11648/j.ajlm.20240901.11},
url = {https://doi.org/10.11648/j.ajlm.20240901.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20240901.11},
abstract = {Thrombocytopenia is defined as a platelet count of less than 150 G/L in the blood. It can be of central or peripheral origin. Newly-formed immature platelets are called reticulated platelets (RP) and are expressed as the immature platelet fraction or IPF. This automated hematological parameter enables us to distinguish between peripheral and central thrombocytopenia in a simple, quick, easily reproducible and non-invasive way. In the present study, our aim was to evaluate the clinical utility of the IPF and its ability to differentiate between central and peripheral thrombocytopenia. In this prospective study, we collected 50 cases of thrombocytopenia in our series. The IPF and all other CBC parameters were measured using the Sysmex XN-1500 analyser. Based on the clinical context and myelogram findings, the subjects in our study were separated into a central thrombocytopenia group and a peripheral thrombocytopenia group. We then assessed variations in IPF between the two groups. The mean IPF in the peripheral thrombocytopenia group was significantly higher than that in the central thrombocytopenia group (15.71 ± 12.02% vs. 5.51 ± 3.04%; p<0.001) and this difference persisted regardless of platelet count. We also established a sensitivity and specificity ROC curve, which showed that the IPF had excellent diagnostic value for differentiating between central and peripheral thrombocytopenia, with an area under the curve of 0.914. We also defined a discriminative cut-off value of 8.5% with a sensitivity of 77.8% and a specificity of 86.4% for defining the origin of thrombocytopenia. Thus, an IPF value above 8.5% points to peripheral thrombocytopenia with increased platelet regeneration. In conclusion, the results of our study have enabled us to formulate recommendations for improving the diagnostic strategy for thrombocytopenia using the immature platelet fraction or IPF.
},
year = {2024}
}
TY - JOUR T1 - Importance of the Immature Platelet Fraction in the Etiological Diagnosis of Thrombocytopenia AU - Mohammed Ali Meskini AU - Kenza El Bazi AU - Hicham Yahyaoui AU - Mohamed Ait Ameur AU - Mohamed Chakour Y1 - 2024/04/29 PY - 2024 N1 - https://doi.org/10.11648/j.ajlm.20240901.11 DO - 10.11648/j.ajlm.20240901.11 T2 - American Journal of Laboratory Medicine JF - American Journal of Laboratory Medicine JO - American Journal of Laboratory Medicine SP - 1 EP - 7 PB - Science Publishing Group SN - 2575-386X UR - https://doi.org/10.11648/j.ajlm.20240901.11 AB - Thrombocytopenia is defined as a platelet count of less than 150 G/L in the blood. It can be of central or peripheral origin. Newly-formed immature platelets are called reticulated platelets (RP) and are expressed as the immature platelet fraction or IPF. This automated hematological parameter enables us to distinguish between peripheral and central thrombocytopenia in a simple, quick, easily reproducible and non-invasive way. In the present study, our aim was to evaluate the clinical utility of the IPF and its ability to differentiate between central and peripheral thrombocytopenia. In this prospective study, we collected 50 cases of thrombocytopenia in our series. The IPF and all other CBC parameters were measured using the Sysmex XN-1500 analyser. Based on the clinical context and myelogram findings, the subjects in our study were separated into a central thrombocytopenia group and a peripheral thrombocytopenia group. We then assessed variations in IPF between the two groups. The mean IPF in the peripheral thrombocytopenia group was significantly higher than that in the central thrombocytopenia group (15.71 ± 12.02% vs. 5.51 ± 3.04%; p<0.001) and this difference persisted regardless of platelet count. We also established a sensitivity and specificity ROC curve, which showed that the IPF had excellent diagnostic value for differentiating between central and peripheral thrombocytopenia, with an area under the curve of 0.914. We also defined a discriminative cut-off value of 8.5% with a sensitivity of 77.8% and a specificity of 86.4% for defining the origin of thrombocytopenia. Thus, an IPF value above 8.5% points to peripheral thrombocytopenia with increased platelet regeneration. In conclusion, the results of our study have enabled us to formulate recommendations for improving the diagnostic strategy for thrombocytopenia using the immature platelet fraction or IPF. VL - 9 IS - 1 ER -
Hematology Laboratory, Avicenna Military Hospital, Marrakech, Morocco
Figure 1. Sysmex XN-1500 in the HMA hematology laboratory.
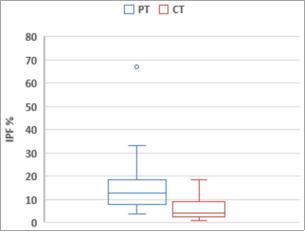
Figure 2. Box plot representing IPF in central thrombocytopenia (CT) and peripheral thrombocytopenia (PT) groups.
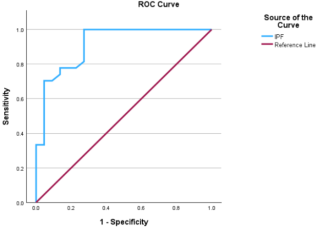
Figure 3. ROC curve showing the sensitivity and specificity of IPF in differentiating between central and peripheral thrombocytopenias.
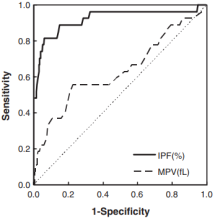
Figure 4. ROC curves in IPF and MPV. The cut-off value was 7,7% with a sensitivity of 86,8% and specificity of 92,6% [18].

Figure 5. Receiver-operating characteristic (ROC) curve of immature platelet fraction (IPF) in the immune thrombocytopenic purpura (ITP) group and non-ITP group. The optimal cut-off value of IPF (%) for differentiating ITP was 7.0% with a sensitivity of 61% and specificity of 70% [21].

